|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
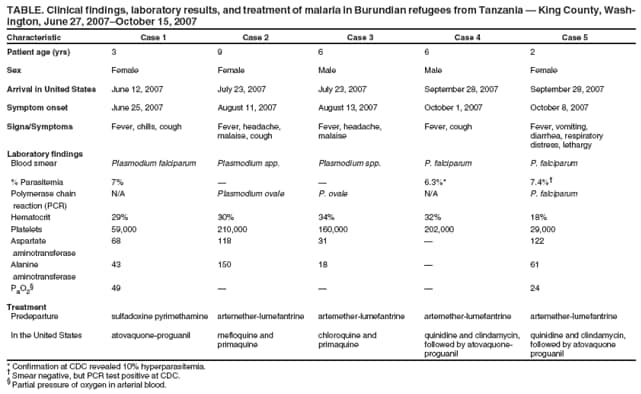
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Malaria in Refugees from Tanzania --- King County, Washington, 2007Recent immigrants and refugees constitute a substantial proportion of malaria cases in the United States, accounting for nearly one in 10 imported malaria cases involving persons with known resident status in 2006 (1). This report describes three cases of Plasmodium falciparum malaria and two cases of Plasmodium ovale malaria that occurred during June 27--October 15, 2007 in King County, Washington. The infections were diagnosed in Burundian refugees who had recently arrived in the United States from two refugee camps in Tanzania. Since 2005, CDC has recommended presumptive malaria treatment with artemisinin-based combination therapy (ACT) (e.g., artemether-lumefantrine) for refugees from sub-Saharan Africa before their departure for the United States (2). Rising levels of resistance to the previous mainstays of treatment, chloroquine and sulfadoxine-pyrimethamine, prompted CDC to make this recommendation. Implementation has been delayed in some countries, including Tanzania, where predeparture administration of presumptive ACT for refugees started in July 2007. The cases in this report highlight the need for health-care providers who care for recently arrived Burundian and other refugee populations to be vigilant for malaria, even among refugees previously treated for the disease. Washington state law requires health-care providers, hospitals, and laboratories to report malaria and certain other conditions to the local health department.* This report summarizes the findings from five cases reported to the local health department by health-care providers and laboratories (Table). After these cases were reported, the patients' medical records were obtained from two local hospitals and reviewed to assist in case investigations. Initial investigations were limited to case investigation forms completed by public health officials based on available medical records. Case 1. A female aged 3 years was diagnosed with P. falciparum malaria in May 2007 while in Tanzania. At that time, she was placed on a quinine-based regimen (formulation, date of administration, and method of administration unknown) and clinically recovered. During an overseas predeparture exam, a requirement for entry into the United States, she received presumptive malaria treatment, with a course of sulfadoxine-pyrimethamine. She arrived in the United States on June 12, 2007, and became ill on June 25, 2007, with fevers, chills, and cough. On June 27, 2007, she was admitted to the local children's hospital. A blood smear revealed 7% hyperparasitemia (>5% = hyperparasitemia) with P. falciparum. Other laboratory findings included anemia, thrombocytopenia, and elevated aspartate aminotransferase. She received oral atovaquone-proguanil, clinically improved, and was discharged July 2, 2007 after 5 days in the hospital. Case 2. A female aged 9 years arrived in the United States on July 23, 2007. Before leaving Tanzania, she received presumptive 3-day treatment of twice daily artemether-lumefantrine; the last doses were administered on July 19, 2007. She became ill on August 11, 2007, with fever, headache, malaise, and cough. She was evaluated in the local county hospital emergency department on August 14, 2007. Blood smear (percent parasitemia unknown) and polymerase chain reaction (PCR) test results were positive for P. ovale. Other laboratory findings included anemia, elevated alanine and aspartate aminotransferase, and hypoalbuminemia. The patient recovered after outpatient treatment with mefloquine and primaquine. Case 3. A male aged 6 years arrived in the United States on July 23, 2007. Before leaving Tanzania, he received presumptive 3-day treatment of twice daily artemether-lumefantrine, with last doses given on July 19, 2007. He became ill on August 13, 2007, with fever, headache, and malaise. He was evaluated in the local county hospital emergency department on August 15, 2007. Laboratory evaluation revealed anemia and P. ovale on blood smear (percent parasitemia unknown) and by PCR. He was treated with chloroquine and primaquine as an outpatient and recovered. Case 4. A male aged 6 years arrived in the United States on September 28, 2007. He received presumptive treatment of artemether-lumefantrine before departure from Tanzania. The last doses were administered on September 24, 2007. He became ill on October 1, 2007, with fever, cough, and decreased energy. He was admitted to a local children's hospital on October 15, 2007. A blood smear revealed P. falciparum with 6.3% hyperparasitemia. Anemia was the other notable laboratory finding. The patient received quinidine and clindamycin, recovered, and was transitioned to atovaquone-proguanil before discharge. He was discharged on October 19, 2007 after spending 4 days in the hospital. Case 5. A female aged 2 years arrived in the United States on September 28, 2007. She received artemether-lumefantrine as presumptive treatment before departure from Tanzania, with the last doses administered on September 24, 2007. She became ill on October 8, 2007, with fever, vomiting, and nonbloody diarrhea. She worsened clinically over the following week, eventually developing respiratory distress and lethargy. She was admitted to the intensive care unit of a local children's hospital on October 15, 2007. Her blood smear revealed 7.4% hyperparasitemia with P. falciparum. Other laboratory findings included anemia, thrombocytopenia, and elevated alanine and aspartate aminotransferase. The patient was treated with quinidine and clindamycin, recovered, and was transitioned to atovaquone-proguanil before discharge on October 19, 2007. She spent a total of 4 days in the hospital. Blood smears from cases 2 through 5 were sent to CDC for confirmation of test results. In cases 2 and 3, blood smears were positive for Plasmodium spp. (without percent parasitemia noted), and PCR was positive for P. ovale. In case 4, the blood smear was notable for a 10% P. falciparum hyperparasitemia. In case 5, the blood smear was negative, but PCR was positive for P. falciparum. Reported by: JS Duchin, MD, TS Kwan-Gett, MD, MPH, S McKeirnan, MPH, M Grandjean, M Ohrt, MPH, S Randels, Public Health--Seattle and King County, Communicable Disease Epidemiology and Immunization Section, Washington. PM Arguin, MD, Malaria Branch, Div of Parasitic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; CR Phares, PhD, Immigrant, Refugee, and Migrant Health Branch, Div of Global Migration and Quarantine, National Center for Preparedness, Detection, and Control of Infectious Diseases; MP Hanson, MD, EIS Officer, CDC. Editorial Note:CDC recommends presumptive treatment of P. falciparum malaria in United States-bound refugees at high risk for infection rather than waiting for development of symptoms and risking severe complications or death after arrival in the United States (2). To be considered adequate presumptive therapy, the regimen must be completed no sooner than 3 days before departure (2). This approach reduces the risk for malaria-related morbidity and mortality among these refugees. Refugees are typically a medically underserved population with difficulty accessing care, which can lead to delays in diagnosis and treatment. Even if refugees are able to obtain care, health-care providers in the United States might not be familiar with recommended malaria treatment regimens. For example, the patient in case 1 did not receive adequate treatment for severe infection with P. falciparum. Instead, she received oral atovaquone-proguanil, which would have been appropriate for uncomplicated malaria. The recommended regimens for severe infection with P. falciparum include either intravenous quinidine or artesunate (3). The latter is available from CDC via an investigational new drug protocol. Presumptive predeparture treatment for malaria in a geographically clustered population of refugees, as in a refugee camp, is easier logistically and less costly than treatment of symptomatic cases dispersed throughout the United States after arrival. Presumptive treatment also can reduce the risk for reintroduction of malaria into the United States. Reintroduction is a concern given that the malaria vector, the female Anopheles mosquito, is widespread in the United States. A recent malaria outbreak in the Caribbean resulting from reintroduction is an example of this possibility (4). The International Organization for Migration (IOM) is an intergovernmental agency that screens and treats most refugees bound for the United States. This is done at the request of the United States in an effort to reduce the incidence of infectious disease among refugees after they reach the United States. IOM administers presumptive treatment against P. falciparum malaria (and intestinal parasites) to refugees resettling from Tanzania before departure for the United States. In 2005, CDC recommended ACT as presumptive P. falciparum treatment for refugees resettling in the United States from sub-Saharan Africa. However, presumptive P. falciparum malaria treatment using sulfadoxine-pyrimethamine was used for Tanzanian refugees until July 7, 2007. CDC surveillance data indicate that among 1,805 Burundian refugees from Tanzania who resettled to 34 U.S. states during May 4--July 7, 2007, 29 symptomatic cases of malaria were identified in 12 states, including Washington. Twenty-six of these refugees (including the patient in case 1) were infected with P. falciparum alone, and two had mixed infections (P. falciparum and P. ovale or Plasmodium malariae). Speciation was not performed for the remaining case. Twenty-four of the 29 (82%) patients were hospitalized; none died (CDC, unpublished data). These 29 refugees departed for the United States before July 7, 2007, the date when IOM implemented the CDC recommendations that refugees from Tanzania receive presumptive treatment with 6-dose artemether-lumefantrine within 3 days before departure for the United States. Instead, they all received sulfadoxine-pyrimethamine before departure; high rates of resistance to sulfadoxine-pyrimethamine have been reported (5), but the artemether-lumefantrine regimen has been effective in field settings in Africa (6). Two of the patients in this report who were infected with P. falciparum, the patients in cases 4 and 5, were resettled to the United States after July 7, 2007, the date when IOM instituted the change to artemether-lumefantrine treatment. These two patients received a complete artemether-lumefantrine presumptive treatment course before departure from Tanzania, yet both were diagnosed with P. falciparum after arrival in the United States. Possible explanations include incomplete treatment or nonadherence to the medication regimen (only 3 of 6 doses were directly observed in these two patients, and in the patients in cases 2 and 3), poor medication absorption, reinfection after treatment, or treatment during a time in the parasite's lifecycle when it would be unaffected by this regimen. In response to such continuing cases, IOM now directly observes all 6 doses of artemether-lumefantrine treatment and provides milk with each dose to improve absorption. Current IOM policy targets infection with P. falciparum only. However, cases 2 and 3 in this series involved relapses of P. ovale after arrival in the United States. Infection with P. ovale (or Plasmodium vivax) generally results in less severe disease than infection with P. falciparum. Hypnozoites of P. ovale or P. vivax can remain dormant in the liver for months or years before causing relapse, and primaquine is the only agent available that can eliminate malaria parasites at this stage of their life cycle (7,8). However, predeparture presumptive treatment with primaquine to prevent relapse of P. ovale or P. vivax currently is not recommended because the cost, logistics of implementing a 14-day medication course, and risk for severe hemolytic anemia in glucose-6-phosphate dehydrogenase (G6PD)--deficient patients outweigh the potential benefit of avoiding a small number of non-P. falciparum malaria cases. Up to 10,000 Burundian refugees from Tanzania will have been resettled in the United States during 2007--2008 (9). Health-care providers in the United States caring for refugee populations resettling from malarial regions should remain aware of the possibility of malaria in these groups, regardless of prior treatment. References
*Notifiable conditions. Ch. 246-101, Washington Administrative Code. Available at http://apps.leg.wa.gov/wac/default.aspx?cite=246-101.
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/13/2008 |
|||||||||
|