|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
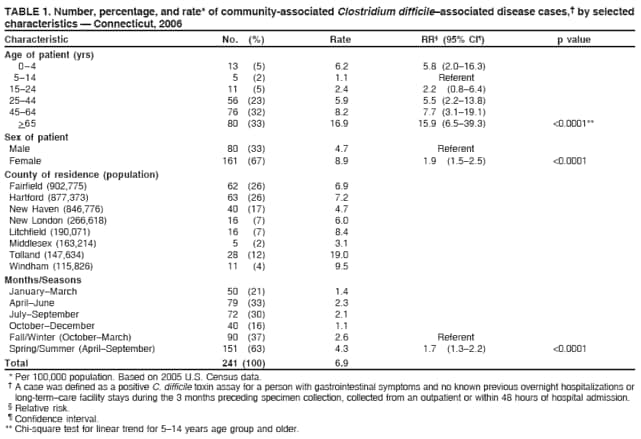
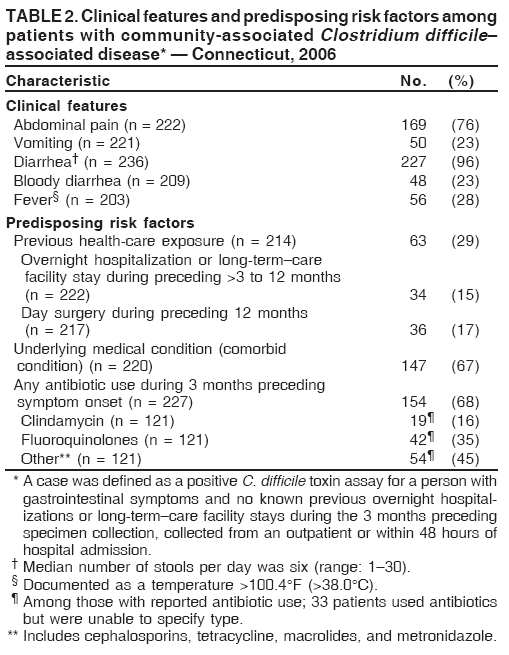
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Community-Associated Clostridium difficile --- Connecticut, 2006Clostridium difficile is a well-known cause of hospital-acquired infectious diarrhea and is associated with increased health-care costs, prolonged hospitalizations, and increased patient morbidity. Previous antimicrobial use, especially use of clindamycin or ciprofloxacin, is the primary risk factor for development of C. difficile--associated diarrhea (CDAD) because it disrupts normal bowel flora and promotes C. difficile overgrowth (1). Historically, CDAD has been associated with elderly hospital in-patients or long-term--care facility (LTCF) residents. Since 2000, a strain of C. difficile that has been identified as North American pulsed-field type 1 (NAP1) and produces an extra toxin (binary toxin) and increased amounts of toxins A and B has caused increased morbidity and mortality among hospitalized patients (2,3). During 2005, related strains caused severe disease in generally healthy persons in the community at a rate of 7.6 cases per 100,000 population, suggesting that traditional risk factors for C. difficile might not always be factors in development of community-associated CDAD (CA-CDAD) (4). Cases of CA-CDAD are not nationally reportable, and population-based data at a statewide level have not been reported previously. In 2006, the Connecticut Department of Public Health (DPH) implemented a statewide surveillance system to assess the burden of CA-CDAD and to determine the descriptive epidemiology, trends, and risk factors for this disease. This report describes that surveillance system and summarizes results from the first year of surveillance. The findings indicated the presence of occasionally severe CDAD among healthy persons living in the community, including persons with no established risk factors for infection. Clinicians should consider a diagnosis of CA-CDAD in outpatients with severe diarrhea, even in the absence of established risk factors. In addition, continued surveillance is needed to determine trends in occurrence and whether more toxigenic strains are having an increasing impact in the community and in the hospital setting. On January 1, 2006, CA-CDAD was added to the list of conditions reportable by Connecticut health-care providers. A case of CA-CDAD was defined as a positive C. difficile toxin assay for a person with gastrointestinal symptoms and no known previous overnight hospitalizations or LTCF stays during the 3 months preceding specimen collection, collected from an outpatient or within 48 hours of hospital admission (5). DPH staff members contacted hospital infection-control practitioners at Connecticut's 32 acute-care hospitals by telephone, informed them about the new reporting requirements, and asked them to review positive laboratory results to identify cases. Laboratories were not required to report to DPH. Physicians were informed by a special mailing. In May 2006, all hospitals were sent a letter summarizing initial findings and reminding physicians and infection-control practitioners about the reporting requirements. In addition, hospitals that did not initially report cases were recontacted by telephone and reminded of the reporting requirements. DPH staff members contacted treating physicians to confirm case status and collect patient information, including demographics, symptoms, select medical history, and possible risk factors. When necessary, DPH staff members reviewed medical records or conducted patient interviews. However, systematic patient interviews to verify absence of a recent stay in a health-care setting were not conducted. Incidence rates were calculated using the number of confirmed cases reported among Connecticut residents and 2005 U.S. Census state population estimates. Differences in proportions and tests for trend by age group were evaluated using the chi-square test and chi-square test for trend; multivariate logistic regression analysis was conducted. A separate 3-month pilot study was conducted during 2006 by FoodNet,* Emerging Infections Program sites,† and CDC to collect specimens from patients with CA-CDAD for culture for C. difficile and to characterize the isolates by toxinotyping and detection of binary toxin and deletions in the tcdC gene (6). As part of this study, in Connecticut, all toxin-positive stool specimens from confirmed CA-CDAD patients at three hospital laboratories were collected and cultured. A total of 456 possible cases, determined on the basis of tests conducted on outpatients or within 2 days of hospitalization, were reported during 2006; 241 (53%) were subsequently confirmed as meeting the case definition. Of the 215 cases that were not confirmed, 159 (74%) occurred in persons who had an LTCF stay or hospitalization during the preceding 3 months, 50 (23%) occurred in persons for whom insufficient medical information was available to enable confirmation; and six (<1%) were in persons who were asymptomatic The overall annual 2006 incidence of CA-CDAD was 6.9 cases per 100,000 population, with similar rates found in most counties. Incidence among those aged >5 years increased with age; females had nearly twice the incidence of males. Rates were higher during the spring and summer months than during the fall and winter months (Table 1). A total of 28 (88%) of 32 acute-care hospitals reported at least one case of CA-CDAD (range: 1--26 cases). Among the 241 cases, 110 (46%) were in patients who required hospitalization for CA-CDAD, mainly for diagnosis and treatment of dehydration or colitis; 13 (12%) were in patients who required an intensive-care unit stay, two (2%) were in patients who had both toxic megacolon and a colectomy, and two (2%) were in patients who died of complications related to C. difficile infection. The median length of stay among hospitalized patients was 4 days (range: 1--39 days). Among all patients for whom follow-up information was available, 29% had an inpatient health-care exposure (defined as overnight hospitalization or LTCF stay during the >3 to 12 months preceding illness or day surgery during the 12 months preceding illness), 67% had an underlying medical condition, and 68% had taken an antimicrobial during the 3 months preceding symptom onset (Table 2). When CA-CDAD patients requiring hospitalization were compared with those managed as outpatients, independent predictors of hospitalization by multivariate analysis included age of >65 years (p = 0.001), fever (p = 0.001), and inpatient health-care exposure during the >3 to 12 months preceding illness (p = 0.04). A total of 59 (25%) patients had no underlying conditions and no inpatient health-care exposures during the 12 months preceding illness. Compared with all other patients, this group was younger (63% versus 23% were aged <45 years [p<0.0001]), less likely to be hospitalized for their CA-CDAD illness (36% versus 52% [p<0.04]), and more likely to report bloody diarrhea (37% versus 19% [p=0.01]). In addition, 35 (59%) patients received an antimicrobial during the 3 months preceding symptom onset, 21 (36%) took no antimicrobial, and three (5%) patients had no information on antimicrobial use available. Twelve C. difficile isolates were recovered from toxin-positive stool specimens and were characterized at CDC. Eight (67%) had binary toxin genes similar to the epidemic NAP1 strain, and three (25%) were identified as NAP1. Coinfection with a second pathogen appeared to be rare. A review of the FoodNet enteric pathogen surveillance database in Connecticut indicated that five (2%) of the 241 patients with CA-CDAD also had a stool-culture positive result for another reportable enteric pathogen from a specimen collected on the same day or within 1 day of the toxin-positive C. difficile sample: Salmonella (one patient), Campylobacter (three), and Escherichia coli O157:H7 (one). Reported by: T Rabatsky-Ehr, MPH, K Purviance, MPH, D Mlynarski, MPH, P Mshar, MPH, J Hadler, MD, Epidemiology and Emerging Infections Program, Connecticut Dept of Public Health. L Sosa, MD, EIS Officer, CDC. Editorial Note:The findings in this report demonstrate that CA-CDAD is an important and geographically widespread health problem among Connecticut outpatients, a population previously thought to be at low risk for this disease. Although interest in CA-CDAD has grown in recent years, this report describes the first attempt to define population-based incidence of this disease at the state level. The CA-CDAD incidence in Connecticut in 2006 (6.9 per 100,000 population) was similar to that found in Philadelphia in 2005 (7.6 per 100,000 population) using a similar case definition. Both of these rates were considerably lower than that found in the United Kingdom (UK) in 2004 (22.0 per 100,000 population), despite the fact the UK study used a more restrictive case definition in which persons with hospitalization during the 12 months preceding illness onset were excluded (4,7). The findings in this report highlight the importance of increasing age (with the attendant underlying health problems and increased use of the health-care system) and antibiotic exposure in the development of CDAD. However, one fourth of all CA-CDAD cases were in persons who lacked established predisposing risk factors for CDAD, including advanced age, an underlying health condition, and a health-care exposure during the 12 months preceding illness. Moreover, similar to what was observed in the community studies conducted in Philadelphia and the UK, 32% of patients had no recent exposure to antimicrobials. Approximately 9% of all cases were in patients who had none of these factors. These findings emphasize the need for continued study of this disease to identify additional risk factors for exposure to C. difficile and for development of disease. The ability of C. difficile to form spores is thought to be a key feature in enabling the bacteria to persist in patients and the physical environment for long periods, thereby facilitating its transmission. C. difficile is transmitted through the fecal-oral route. Postulated risk factors for acquiring C. difficile in the community include contact with a contaminated health-care environment, contact with persons who are infected with and shedding C. difficile (person-to-person transmission), and ingestion of contaminated food. Studies have shown C. difficile to be a pathogen or colonizer of calves, pigs, and humans (8,9). The recent detection of the NAP1 strain of C. difficile in retail ground beef is cause for concern (9). This hyper--toxin-producing strain has been reported as a cause of serious outbreaks of health-care--associated disease in humans in North America and Europe (10) and was found among a small subset of specimens from CA-CDAD cases in Connecticut. Further studies are needed to determine whether C. difficile is transmitted via the food chain and the relative importance of such transmission in human CDAD. The findings in this report are subject to at least four limitations. First, measured incidence is subject to the limitations of the toxin-detection assays usually used for diagnosis of C. difficile. These assays can be insensitive (i.e., 65%--90% sensitivity) and nonspecific; in addition, 1%--2% of persons tested with the most widely used toxin assays might test positive in the absence of infection. Because C. difficile is difficult and labor-intensive to isolate, culture usually is only used when a clinical need for verification of a positive toxin assay exists. Second, because systematic patient interviews were not conducted, some patients might have had recent health-care exposures that were not recorded in available medical records, leading to potential misclassification of health-care--associated cases as CA-CDAD. Third, underreporting might have occurred because laboratories were not required to report and no validation or assessment of completeness of reporting was conducted. Finally, because cultures were not routinely collected for isolation and molecular characterization of organisms, the extent to which recently described emerging strains are causing disease in Connecticut or are responsible for illness in persons without established risk factors for CA-CDAD is unknown. Future CA-CDAD surveillance measures in Connecticut will focus on collecting detailed information on hospitalized patients for whom more complete medical records are available. Continued population-based surveillance is necessary to monitor trends and describe the extent of CA-CDAD and possible risk factors. Although CA-CDAD surveillance systems are resource intensive, other states should consider implementing these systems to assess trends in CA-CDAD and to help health-care providers become more aware of this emerging problem. Acknowledgments This report is based, in part, on data contributed by the Yale University Emerging Infections Program, New Haven; laboratory staff members at the Hospital of St. Raphael, New Haven, Connecticut; and members of CDC's FoodNet. References
* The Foodborne Diseases Active Surveillance Network (FoodNet) is the principal foodborne and enteric disease surveillance component of CDC's Emerging Infections Program (EIP). FoodNet is a set of population-based surveillance projects for laboratory-confirmed disease collaboratively undertaken by CDC, 10 EIP sites (Connecticut, Georgia, Maryland, Minnesota, New Mexico, Oregon, Tennessee, and selected counties in California, Colorado, and New York), the U.S. Department of Agriculture, and the Food and Drug Administration. † The CDC Emerging Infections Program supports population-based surveillance in 10 sites in the United States. Each site is based in a state health department, often with a local academic center partner, working in collaboration with local health departments, public health laboratories, clinical laboratories, infection-control practitioners, health-care providers, and hospitals to assess the public health impact of emerging infections and evaluate methods for their prevention and control. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/2/2008 |
|||||||||
|