|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
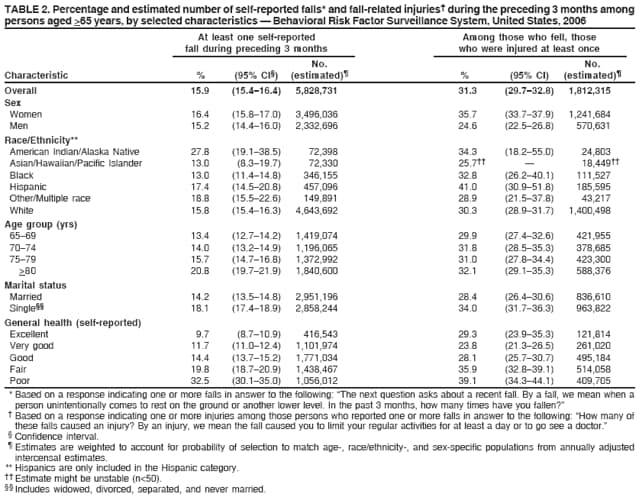
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Self-Reported Falls and Fall-Related Injuries Among Persons Aged >65 Years --- United States, 2006Each year, an estimated one third of older adults fall, and the likelihood of falling increases substantially with advancing age. In 2005, a total of 15,802 persons aged >65 years died as a result of injuries from falls (1). However, the number of older adults who fall and are not injured or who sustain minor or moderate injuries and seek treatment in clinics or physician offices is unknown. To estimate the percentage of older adults who fell during the preceding 3 months, CDC analyzed data from the 2006 Behavioral Risk Factor Surveillance System (BRFSS) survey. This report summarizes the results of that analysis, which indicated that approximately 5.8 million persons aged >65 years, or 15.9% of all U.S. adults in that age group, fell at least once during the preceding 3 months, and 1.8 million (31.3%) of those who fell sustained an injury that resulted in a doctor visit or restricted activity for at least 1 day. The percentages of women and men who fell during the preceding 3 months were similar (16.4% versus 15.2%, respectively), but women reported significantly more fall-related injuries than men (35.7% versus 24.6%, respectively). The effect these injuries have on the quality of life of older adults and on the U.S. health-care system reinforces the need for broader use of scientifically proven fall-prevention interventions. BRFSS surveys are conducted in all 50 states, the District of Columbia (DC), and selected U.S. territories (Puerto Rico, the U.S. Virgin Islands, and Guam) (2). BRFSS uses a multistage sampling design based on random-digit--dialing methods to select a representative sample of the noninstitutionalized, civilian population aged >18 years in each state or territory. Details on the design, random sampling procedures, and reliability and validity of measures used in BRFSS have been described previously (3,4). In 2006, the median response rate among states, based on Council of American Survey Research Organizations (CASRO) guidelines, was 51.4% (range: 35.1%--66.0%). Data were weighted to account for probability of selection and to match the age-, race/ethnicity-, and sex-specific populations from annually adjusted intercensal estimates. Statistical significance was determined by nonoverlap of 95% confidence intervals. Estimates were considered unstable if the unweighted sample size for the subgroup was less than 50. In 2006, interviews with 92,808 persons aged >65 years were completed. Data from all 50 states, DC, Puerto Rico, and the U.S. Virgin Islands are included in this report. Two questions about falls were included in the 2006 survey. The first was, "The next question asks about a recent fall. By a fall, we mean when a person unintentionally comes to rest on the ground or another lower level. In the past 3 months, how many times have you fallen?" Those who reported a fall were asked a second question, "How many of these falls caused an injury? By an injury, we mean the fall caused you to limit your regular activities for at least a day or to go see a doctor." In response to the first question, the number of reported falls ranged from 0 to 76; the mean number of falls among those who fell was 1.9; median = 1.0. Of respondents who said they had fallen, 23.1% reported falling three times or more. Overall, 15.9% of respondents reported one or more falls (Table 1). The number of reported falls that resulted in injury ranged from 0 to 50. Among those who fell and were injured, the mean number of injurious falls was 1.4; median = 1.0. Overall, 31.3% of respondents who reported falling also reported a fall-related injury. The percentages of men and women who reported falling during the preceding 3 months were similar (15.2% and 16.4%, respectively) (Table 2), but women reported more fall-related injuries than men (35.7% versus 24.6%). By race/ethnicity, American Indians/Alaska Natives reported the greatest percentage of falls (27.8%); Hispanics reported the greatest percentage of falls with injuries (41.0%). The percentages of persons aged 65--69 years and 70--74 years who reported falling during the preceding 3 months were similar (13.4% versus 14.0%) but increased significantly for persons aged 75--79 years (15.7%) and >80 years (20.8%). Although the percentage of persons reporting falls increased with age, the percentage of persons reporting fall-related injuries was nearly identical for each age group (range: 29.9%--32.1%). Reports of falls ranged from 12.8% among respondents in Hawaii to 20.1% among those in Vermont, but no geographic patterns were apparent. The 50 states and DC were ranked according to their age-adjusted fall mortality rates for 2003--2004. Of the seven states at or above the 90th percentile nationally (Arizona, Minnesota, New Mexico, Rhode Island, South Dakota, Vermont, and Wisconsin) (1), only Vermont (first) and New Mexico (seventh) also were among the 10 states with the greatest proportion of reported falls; only Rhode Island (first) and Arizona (seventh) appeared among the 10 states with the greatest proportion of fall-related injuries. The percentage of respondents who fell and were injured ranged from 23.7% (Nebraska) to 48.0% (Rhode Island). Reported by: JA Stevens, PhD, KA Mack, PhD, LJ Paulozzi, MD, MF Ballesteros, PhD, Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control, CDC. Editorial Note:Falls are the leading cause of fatal and nonfatal injuries for persons aged >65 years (1). National estimates for rates of fatal falls and fall-related injuries treated in emergency departments have been published previously (1); however, this report presents the first national estimates of the number and proportion of persons experiencing fall-related injuries associated with either restricted activity or doctor visits. The results in this study suggest that in 2006, approximately 1.8 million persons aged >65 years (nearly 5% of all persons in that age group) sustained some type of recent fall-related injury. Even when those injuries are minor, they can seriously affect older adults' quality of life by inducing a fear of falling, which can lead to self-imposed activity restrictions, social isolation, and depression (5). In addition, fall-related medical treatment places a burden on U.S. health-care services. In 2000, direct medical costs for fall-related injuries totaled approximately $19 billion (6). A recent study determined that 31.8% of older adults who sustained a fall-related injury required help with activities of daily living as a result, and among them, 58.5% were expected to require help for at least 6 months (7). Few studies of falls have used a 3-month time frame, so comparison with other studies is challenging. A recent analysis of data from the National Health Interview Survey (NHIS) presented the number and rate of medically attended falls reported during the preceding 3 months. However, the NHIS design did not permit calculation of the number of persons injured (7). Among persons aged >65 years, other studies have reported that women fall more frequently and are treated for fall-related injuries, especially fractures, more often than men (8). Similarly, the analysis of BRFSS data indicated that a greater proportion of women than men reported fall-related injuries, but it did not find a significant difference between the proportion of women and men that experienced falls. The reasons for the differences in results between these studies are uncertain. Women might be less likely than men to report a noninjurious fall, or more likely than men to restrict their activities or seek medical attention after a fall. The BRFSS definition of a fall-related injury does not specify severity; an injury could be as minor as a small bruise or as severe as a broken hip. This broad definition could have obscured age-related differences if, for example, persons aged 65--69 years sustained less severe injuries and persons aged >80 years experienced more severe injuries. The findings in this report are subject to at least five limitations. First, BRFSS is a telephone-based survey and excludes households without landline telephones, so the results might be subject to selection bias. Second, data are self-reported and subject to recall bias; therefore, prevalence estimates of falls might be underestimated. Third, BRFSS does not include institutionalized persons, thereby excluding persons in long-term--care facilities, who are most at risk for falls. Fourth, the broad definition of injury might have led participants to report minor falls as injurious, resulting in an estimate of fall-related injuries that is higher than in other similar studies. Finally, the low response rate and possible response bias might have affected the representativeness of these data. Falls and fall-related injuries seriously affect older adults' quality of life and present a substantial burden to the U.S. health-care system. Modifiable fall risk factors include muscle weakness, gait and balance problems, poor vision, use of psychoactive medications, and home hazards (8). Falls among older adults can be reduced through evidence-based fall-prevention programs that address these modifiable risk factors. Most effective interventions focus on exercise, alone or as part of a multifaceted approach that includes medication management, vision correction, and home modifications (8). One example of an effective fall-prevention program is "Moving for Better Balance," a Tai Chi program based on a randomized controlled trial conducted at the Oregon Research Institute, which reduced the frequency of falls by 55% (9). The program is conducted in senior centers in Oregon; participants learn eight body-movement exercises during 1-hour classes offered twice weekly for 12 weeks. This program and 13 other proven fall-prevention strategies are described in a new publication, Preventing Falls: What Works. A Compendium of Effective Community-Based Interventions from Around the World. The companion publication, Preventing Falls: How to Develop Community-Based Fall Prevention Programs for Older Adults, offers guidelines to help organizations develop fall-prevention programs. These publications and other fall-related educational materials are available at http://www.cdc.gov/ncipc/duip/fallsmaterial.htm. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/5/2008
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|