|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
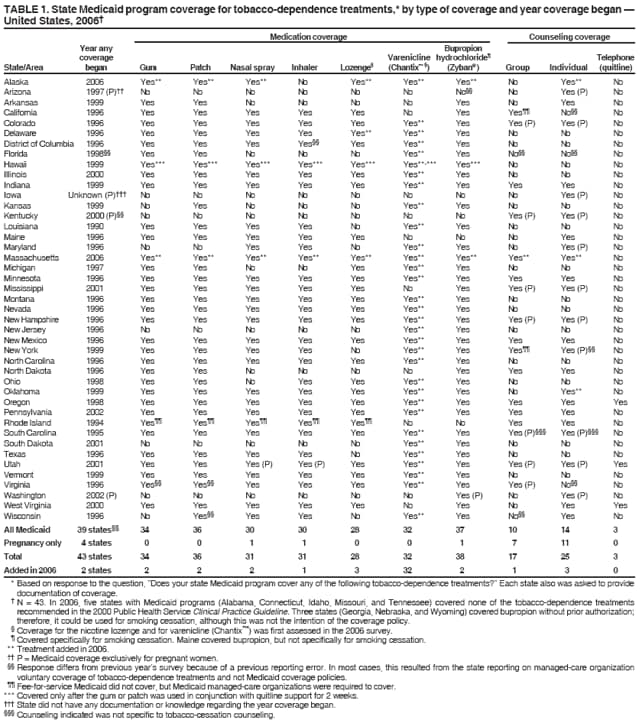
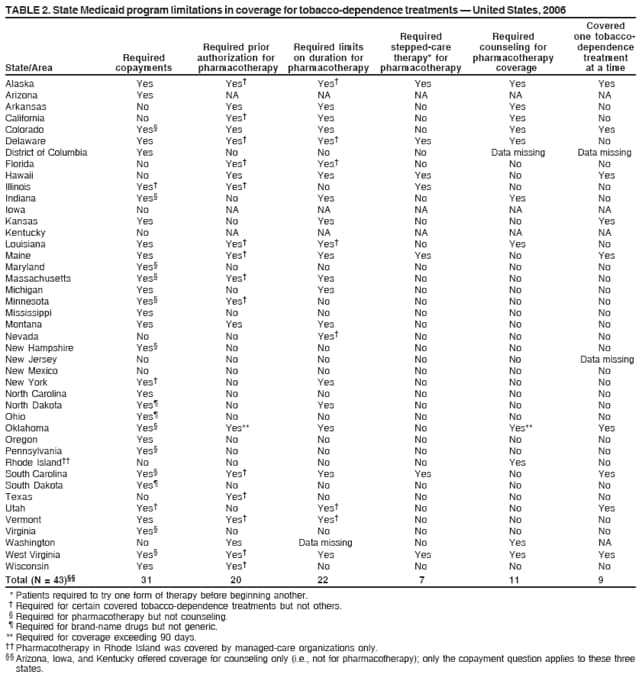
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. State Medicaid Coverage for Tobacco-Dependence Treatments --- United States, 2006Approximately one third of adult Medicaid recipients smoke (1). The Public Health Service (2), the Task Force on Community Preventive Services (3), and the Institute of Medicine (4) recommend that health-insurance coverage be provided for tobacco-dependence treatments. In addition, a Healthy People 2010 national health objective calls for total health-insurance coverage for evidence-based tobacco-dependence treatments in all 51 Medicaid programs (objective 27-8b) (5). The types of tobacco-dependence treatments covered by Medicaid have been reported periodically from surveys conducted by the Center for Health and Public Policy Studies at the University of California, Berkeley (6). This report summarizes results of the 2006 survey, which determined that 39 state Medicaid programs (including the District of Columbia) covered some form of tobacco-dependence treatment (i.e., medication or counseling) for all Medicaid recipients and one state program provided coverage for all recommended treatments. Two states that previously provided no coverage for tobacco-dependence treatment began coverage in 2006. In addition, 32 states added coverage for a new medication, varenicline (Chantix™ [Pfizer, Mission, Kansas]), one state expanded its coverage to include the nicotine lozenge, and one state expanded coverage to include individual counseling. If the 2010 objective is to be achieved, Medicaid coverage for tobacco-dependence treatment must increase substantially. In October 2006, state Medicaid program directors were asked to identify staff members who were most knowledgeable about coverage and programs for tobacco-dependence treatment, and a survey was e-mailed to the identified staff member in each state. Follow-up was conducted through telephone, e-mail, and fax; the response rate was 100%. The survey included questions regarding coverage of tobacco-dependence treatments, the year coverage was first offered, treatments offered to pregnant women, and program requirements for patient copayments or limitations on use of treatments. The 2006 survey, for the first time, included a question regarding coverage for the nicotine lozenge and varenicline (Chantix). Medicaid programs also were asked to submit either a written copy of their coverage policies for tobacco-dependence treatments or a copy of related documentation. Of the 43 programs that reported offering coverage in 2006, a total of 41 provided some supporting documentation: 23 provided detailed documentation matching their survey responses (although seven were missing documentation regarding Chantix), 17 provided partial benefit information (e.g., documentation for pharmacotherapy but not counseling), and one provided general benefit information (i.e., mentioned coverage but did not specify which treatments were covered). A total of 39 (76.5%) Medicaid programs reported offering coverage for at least one form of tobacco-dependence treatment for their entire Medicaid population (Table 1). In addition, four states reported offering coverage for pregnant women only. Of the 39 programs that offered any coverage to their entire Medicaid population, all covered some pharmacotherapy: Zyban® (GlaxoSmithKline, Research Triangle Park, North Carolina) or its generic equivalent (bupropion) (37 programs), nicotine patches (36), nicotine gum (34), varenicline (Chantix) (32), nicotine nasal spray (30), nicotine inhalers (30), and nicotine lozenges (28). Seventeen states covered some form of tobacco-cessation counseling services for their entire Medicaid population (Table 1). An additional 10 states covered counseling services for pregnant women only. Of the 17 states that covered group counseling, 10 covered it for all their Medicaid enrollees, and seven covered group counseling for pregnant women only. Of the 25 states that covered individual counseling, 14 covered the entire population, and 11 covered individual counseling for pregnant women only. The three states that covered telephone counseling covered it for their entire Medicaid population. From 2005 to 2006, two states (Alaska and Massachusetts) added coverage, one state (Delaware) expanded existing coverage to include the nicotine lozenge, and one state (Oklahoma) expanded existing coverage to include individual counseling. Varenicline (Chantix), which was approved by the Food and Drug Administration (FDA) as a tobacco-dependence treatment in 2006, was added as a covered benefit in 32 states. No state added coverage for telephone counseling in 2006. In three states (California, New York, and Rhode Island), tobacco-dependence treatments were covered for enrollees in Medicaid managed-care organizations but not for those in fee-for-service Medicaid programs. For example, in Rhode Island, a legislative mandate for coverage of tobacco-dependence treatment in managed-care organizations resulted in coverage for all forms of nicotine-replacement therapy for enrollees in Medicaid managed-care organizations, whereas fee-for-service enrollees were covered for counseling services only.* Many Medicaid programs had limitations on coverage of tobacco-dependence treatment, including copayments, requirements for prior authorization to obtain coverage, limitations on treatment duration, requirements that patients try one form of therapy before beginning another (i.e., stepped-care therapy), and provision of coverage for one type of tobacco-dependence treatment at a time. Requiring copayments for tobacco-dependence treatments was the most common limitation among Medicaid programs. Among the 43 programs that covered any tobacco-dependence treatments (either for all recipients or for pregnant women), 72% required copayments (Table 2); 14 required copayments for all covered tobacco-dependence treatments (medications and counseling), and 17 required copayments for specific tobacco-dependence treatments, including 11 states that required copayments for all types of pharmacotherapy but none for counseling, three states that required copayments for brand-name tobacco-dependence drugs but not for generic drugs, and three states that required copayments for certain, but not all, medications. Among the 40 programs covering any generic drugs for tobacco-dependence treatment, 26 (65%) required copayments for generic drugs (median: $2 per prescription; range: $1--$5). Of the 40 programs covering any brand-name drugs for tobacco-dependence treatment, 30 (75%) required copayments (median: $3; range: $1--$15). Of the 27 programs covering counseling, five (19%) required copayments (median: $2; range: $1--$3) for these services. Prior authorization for tobacco-dependence treatments was required by 20 states, with six states requiring prior authorization for all pharmacologic tobacco-dependence treatments and 14 states requiring prior authorization for selected treatments (Table 2). Twenty-two Medicaid programs had limitations on the duration of treatment for medications (median: 12 weeks). Twenty-one had limitations on the number of courses of pharmacologic treatment per year (median: one course); four programs (Colorado, Louisiana, Montana, and North Dakota) applied these limits to a lifetime benefit. Seven state Medicaid programs used stepped-care therapy, which requires use of a specific tobacco-dependence treatment before any other treatments are covered. Eleven states required enrollees to participate in counseling services to be eligible for pharmacotherapy coverage, even though two of these programs did not cover counseling. Nine states reported that Medicaid paid for one tobacco-dependence medication at a time. Reported by: HA Halpin, PhD, SB McMenamin, PhD, CA Cella, MPH, NM Bellows, PhD, Center for Health and Public Policy Studies, School of Public Health, Univ of California, Berkeley. CG Husten, MD, Office on Smoking and Health, CDC. Editorial Note:Ten percent of U.S. smokers have a tobacco-related disease (7). Each year, tobacco use in the United States results in $193 billion in health-care costs and lost productivity (8), including an estimated 14% of Medicaid costs (9). Approximately 35% of adult Medicaid recipients were current smokers in 2006 (1). Effective tobacco-dependence treatments include FDA-approved pharmacotherapy and individual, group, and telephone counseling (2). Evidence indicates that tobacco-dependence treatment is highly cost-effective, even cost-saving, in certain populations (10). Nonetheless, certain states might be reluctant to add a new Medicaid benefit when facing state Medicaid budget cuts. In 2006, eight states provided no Medicaid coverage for tobacco-dependence treatments, only seven states covered all FDA-approved medications and at least one form of counseling for all enrollees, and only one state (Oregon) covered all treatments recommended by the Clinical Practice Guideline (2). In 2006, measures that limited use of tobacco-dependence treatments among Medicaid beneficiaries were common, including measures that were inconsistent with the guideline (i.e., copayments, stepped-care approaches, requirements for enrollment in counseling to obtain medication, limitations on number of treatment courses, and not allowing combined treatments) (2,3). Only New Mexico had medication-coverage policies for the entire Medicaid population consistent with current guideline recommendations to reduce barriers to tobacco-dependence treatment. The findings in this report are subject to at least two limitations. First, although all but two states provided some supporting documentation, only 37% provided complete documentation of all covered treatments. Lack of confirmatory documentation for any self-reported data increases the likelihood of reporting errors. Second, certain percentages of Medicaid coverage in this report might differ from those in previous survey years because of previous reporting errors, not because coverage levels changed. In most cases, this resulted from particular states reporting data on managed-care organization voluntary coverage of tobacco-dependence treatments and not on Medicaid coverage policies. Community and policy interventions that increase tobacco-use cessation include increasing the price of tobacco products, sustained media campaigns that encourage cessation and provide information about available treatments, comprehensive smoke-free policies in workplaces and public places, and state-funded tobacco-cessation quitlines (3). Although free, proactive counseling services might be available to Medicaid enrollees through state quitlines, and certain quitlines provide pharmacotherapy to Medicaid enrollees, many state quitlines do not have the capacity to provide comprehensive services (8). Thus, Medicaid partnerships with the state quitlines and coverage for telephone counseling and medications can help ensure that Medicaid recipients receive the services that will maximize their chances of quitting successfully. Recently, the Institute of Medicine (IOM) called for eliminating all tobacco use in the United States (4). In addition to recommending regulation of tobacco products and full funding of comprehensive tobacco prevention and control programs at the CDC-recommended level, IOM specifically called for all insurance, managed-care, and employee benefit plans, including Medicaid, to cover reimbursement for effective smoking-cessation programs. Fully covering all recommended tobacco-dependence treatments, eliminating restrictions and barriers to using treatments, promoting treatment use, and educating Medicaid recipients and providers about coverage are all critical to reducing tobacco use. References
* Additional information available at http://www.rilin.state.ri.us/publiclaws/law06/law06262.htm.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/6/2008 |
|||||||||
|