|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
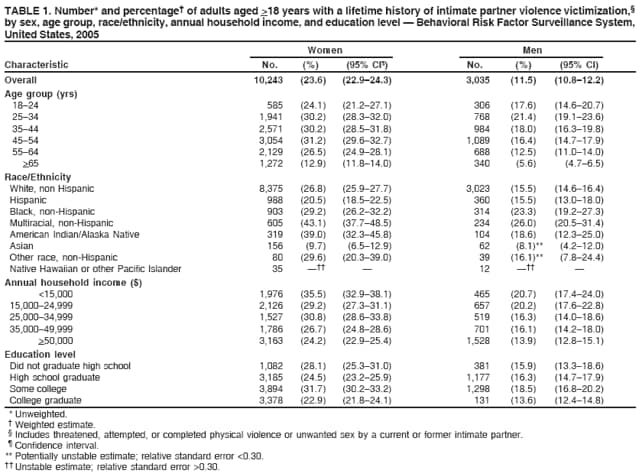
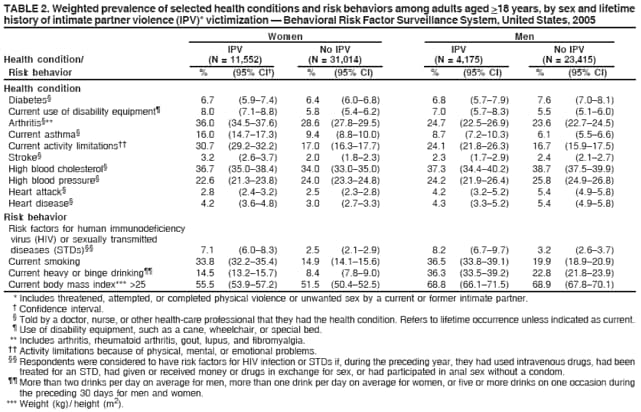
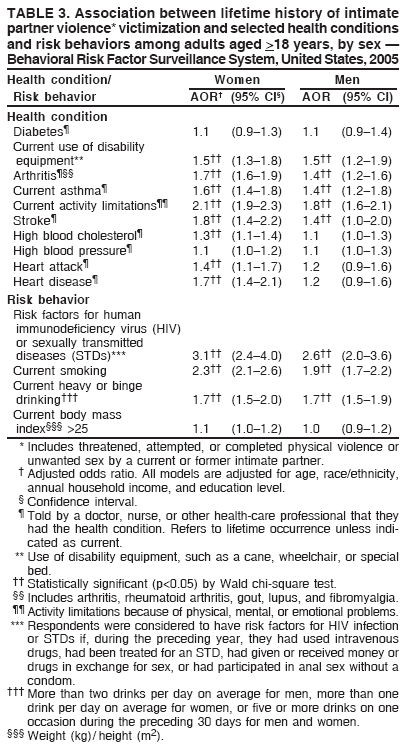
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Adverse Health Conditions and Health Risk Behaviors Associated with Intimate Partner Violence --- United States, 2005An erratum has been published for this article. To view the erratum, please click here. Intimate partner violence (IPV) is defined as threatened, attempted, or completed physical or sexual violence or emotional abuse by a current or former intimate partner. IPV can be committed by a spouse, an ex-spouse, a current or former boyfriend or girlfriend, or a dating partner (1). Each year, IPV results in an estimated 1,200 deaths and 2 million injuries among women and nearly 600,000 injuries among men (1). In addition to the risk for death and injury, IPV has been associated with certain adverse health conditions and health risk behaviors (1). To gather additional information regarding the prevalence of IPV and to assess the association between IPV and selected adverse health conditions and health risk behaviors, CDC included IPV-related questions in an optional module of the 2005 Behavioral Risk Factor Surveillance System (BRFSS) survey. This report describes the results of that survey, which indicated that persons who report having experienced IPV during their lifetimes also are more likely to report current adverse health conditions and health risk behaviors. Although a causal link between IPV and adverse health conditions cannot be inferred from these results, they underscore the need for IPV assessment in health-care settings. In addition, the results indicate a need for secondary intervention strategies to address the health-related needs of IPV victims and reduce their risk for subsequent adverse health conditions and health risk behaviors. BRFSS is an annual, state-based, random-digit--dialed telephone survey of the noninstitutionalized, U.S. civilian population aged >18 years. The survey solicits information on a range of health conditions and health risk behaviors. Data are weighted to account for probability of selection and to match the age-, race/ethnicity-, and sex-specific populations from annually adjusted intercensal estimates. In 2005, a total of 70,156 respondents (42,566 women and 27,590 men) in 16 states and two territories* completed the optional IPV module. Among these 18 states/territories, the median response rate for the 2005 BRFSS core survey, based on Council of American Survey and Research Organizations (CASRO) guidelines, was 51.6% (range: 37.8% [Massachusetts] to 72.7% [Puerto Rico]). The design and characteristics of BRFSS have been described previously.† Logistic regression models were stratified by sex and included age, race/ethnicity, annual household income, and education level as control variables. Statistical significance (p<0.05) was determined using the Wald chi-square test. The IPV module included four questions regarding physical or sexual violence by a current or former intimate partner that respondents had experienced during their lifetimes. Respondents were classified as having experienced IPV if they reported that any of the following had occurred during their lifetimes: threatened, attempted, or completed physical violence or unwanted sex by a current or former intimate partner.§ Health conditions and risk behaviors were selected to cover the full range of conditions and behaviors assessed by BRFSS. These included two self-reported health conditions: 1) current use of disability equipment (e.g., a cane, wheelchair, or special bed) and 2) current activity limitations because of physical, mental, or emotional problems. Respondents also were asked whether they had ever been told by a doctor, nurse, or other health-care professional that they had 1) high blood cholesterol; 2) nongestational high blood pressure; 3) nongestational diabetes; 4) cardiovascular disease (e.g., heart attack, angina, coronary heart disease, or stroke); 5) joint disease (e.g., arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia); or 6) current asthma. In addition, selected health risk behaviors were assessed: 1) risk factors for human immunodeficiency virus (HIV) infection or sexually transmitted diseases (STDs) (i.e., if, during the preceding year, respondent had used intravenous drugs, had been treated for an STD, had given or received money or drugs in exchange for sex, or had participated in anal sex without a condom); 2) current smoking; 3) heavy or binge alcohol use (i.e., more than two drinks per day on average for men, more than one drink per day on average for women, or five or more drinks on one occasion during the preceding 30 days for men and women); and 3) having a body mass index (BMI) (weight [kg]/ height [m2]) >25.¶ Lifetime IPV prevalence estimates were calculated by sex, age group, race/ethnicity, annual household income, and education level (Table 1). Lifetime IPV prevalence was significantly higher (p<0.05) among women than among men; higher among multiracial, non-Hispanic, and American Indian/Alaska Native women; and higher among lower-income respondents. The prevalence of each health condition and risk behavior was calculated by sex of the respondent and lifetime experience of IPV (Table 2). In addition, associations between lifetime IPV and health conditions and risk behaviors were assessed in individual logistic regression models, controlling for age, race/ethnicity, annual household income, and education level (Table 3). With the exceptions of diabetes, high blood pressure, and BMI >25, reporting of health conditions and risk behaviors was significantly higher among women who had experienced IPV during their lifetimes compared with women who had never experienced IPV. Among women, adjusted odds ratios ranged from 1.3 (95% confidence interval [CI] = 1.1--1.4) for high blood cholesterol to 3.1 (CI = 2.4--4.0) for risk factors for HIV infection or STDs (Table 3). Men who had experienced IPV during their lifetimes had a significantly higher prevalence of the following: use of disability equipment, arthritis, asthma, activity limitations, stroke, risk factors for HIV infection or STDs, smoking, and heavy or binge drinking. Adjusted odds ratios ranged from 1.4 (CI = 1.0--2.0) for stroke to 2.6 (CI = 2.0--3.6) for risk factors for HIV infection or STDs (Table 3). Reported by: MC Black, PhD, MJ Breiding, PhD, National Center for Injury Prevention and Control, CDC. Editorial Note:The findings in this report are similar to those of other studies that have linked IPV with poor general health, chronic disease, disability, somatic syndromes, injury, chronic pain, STDs, functional gastrointestinal disorders, and changes in endocrine and immune functions (2--5). However, these studies often lacked the power to analyze individual outcomes and were limited to examining broader health indices. The sample size in this study is approximately four times larger than any previous health study of IPV in the United States and included a range of adverse health conditions and behaviors. Because BRFSS is a cross-sectional survey, these findings cannot address causality. For example, whether adverse health outcomes are caused by IPV cannot be inferred. Evidence from other studies, however, suggests that one underlying mechanism that might link IPV and chronic diseases is the biologic response to long-term or ongoing stress (2--5). For example, the link between violence, stress, and somatic disorders (e.g., fibromyalgia, chronic fatigue syndrome, temporomandibular disorder, and irritable bowel syndrome) has been well established (3,5). These same stress responses also have been linked to various chronic diseases, including cardiovascular disease, asthma, diabetes, and gastrointestinal disorders (3,6). Conversely, adverse health conditions might, in certain cases, lead to increased IPV. Data suggest that women with disabilities experience more IPV than those without disabilities (7). The findings in this report are subject to at least three other limitations. First, because BRFSS is a telephone survey of residential households, persons without landline telephones (i.e., those with no telephone or with a cellular telephone only) are not represented in the sample. Second, because not all states/territories administered the IPV module, the data might not be representative of the entire U.S. adult population. Finally, although these findings indicated an association between IPV and adverse health conditions and health risk behaviors, not all persons who experience IPV would be expected to experience these conditions and behaviors. The number and range of questions that could be included in the IPV module were limited, and information was not collected on the severity, frequency, and context of IPV experienced by respondents. These important factors likely would influence the observed association between IPV and adverse health conditions and health risk behaviors. Whether IPV is followed by adverse health conditions or adverse health conditions lead to IPV, both are likely to affect the overall health of affected persons, suggesting that clinicians should consider assessing exposure to IPV when patients have signs or symptoms of stress or other conditions that are consistent with IPV. Such assessment might influence the diagnosis, treatment plan, and ability of the patient to adhere to treatment. Assessing exposure to IPV as part of good clinical practice is included in the recommendations of several medical organizations, including the American Medical Association (8) and the American College of Obstetricians and Gynecologists (9). CDC recently published Intimate Partner Violence and Sexual Violence Victimization Assessment Instruments for Use in Healthcare Settings (10). This compilation includes an inventory of tools that can be used by health-care providers to determine whether a patient is a victim of IPV or sexual violence and to identify those patients requiring additional services or referrals. References
* States: Arizona, Hawaii, Iowa, Maine, Michigan, Missouri, Nebraska, New Mexico, Nevada, Ohio, Oklahoma, Oregon, Rhode Island, Vermont, Virginia, and Washington. Territories: Puerto Rico and the U.S. Virgin Islands. † CDC. Behavioral Risk Factor Surveillance System 2005 summary data quality report. Available at http://ftp.cdc.gov/pub/data/brfss/2005summarydataqualityreport.pdf. § Respondents were classified as having experienced IPV if they responded "yes" to any of the following four questions: 1) "Has an intimate partner ever threatened you with physical violence? This includes threatening to hit, slap, push, kick, or hurt you in any way." 2) "Has an intimate partner ever attempted physical violence against you? This includes times when they tried to hit, slap, push, kick, or otherwise hurt you, but they were not able to." 3) "Has an intimate partner ever hit, slapped, pushed, kicked, or hurt you in any way?" and 4) "Have you ever experienced any unwanted sex by a current or former intimate partner? Unwanted sex includes things like putting anything into your vagina [if respondent was female], anus, or mouth, or making you do these things to them after you said or showed that you didn't want to. It includes times when you were unable to consent, for example, when you were drunk or asleep, or you thought you would be hurt or punished if you refused." An intimate partner was defined to include any current or former spouse, boyfriend, girlfriend, or dating partner or any person with whom the respondent had ever been romantically or sexually intimate. ¶ CDC. Behavioral Risk Factor Surveillance System 2005 survey questions. Available at http://www.cdc.gov/brfss/questionnaires/pdf-ques/2005brfss.pdf.
Table 1
All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/6/2008 |
|||||||||
|