|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
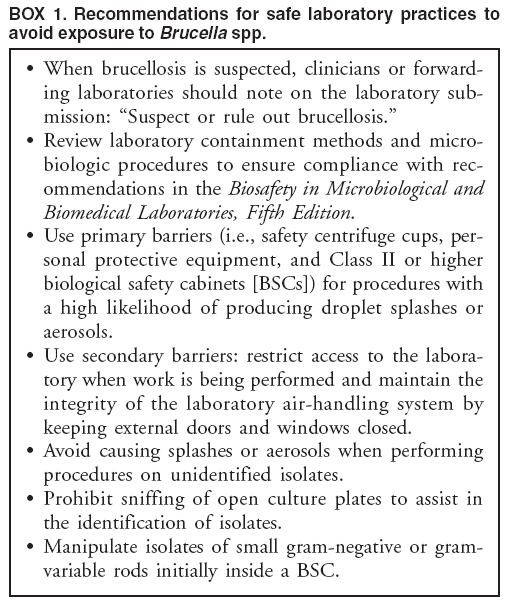
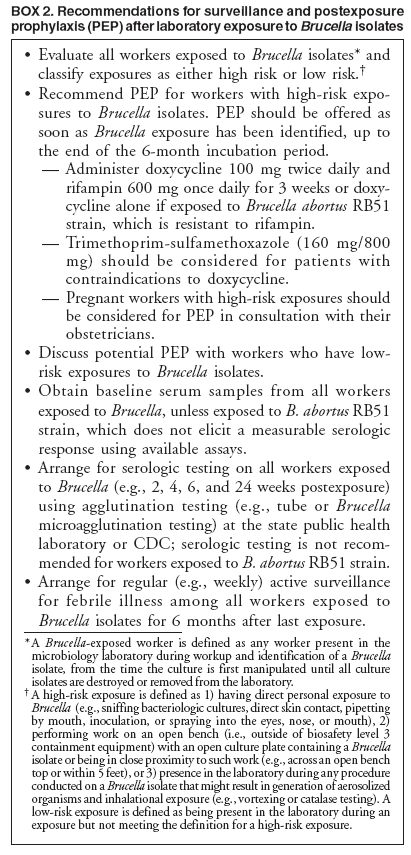
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Laboratory-Acquired Brucellosis --- Indiana and Minnesota, 2006In November 2006, two cases of brucellosis in microbiologists at two clinical laboratories were reported to state health departments in Indiana and Minnesota. The Minnesota Department of Health (MDH) contacted CDC regarding this suspected multistate cluster of laboratory-acquired brucellosis. MDH and the Indiana State Department of Health (ISDH) asked CDC to conduct further testing on Brucella isolates suspected of causing the infections and to provide recommendations for appropriate response by the laboratories. This report summarizes the investigation conducted jointly by MDH, ISDH, and CDC, provides guidance on safe laboratory handling of Brucella spp., and makes recommendations for responding to Brucella laboratory exposures. The results of that investigation determined that 146 workers at the two laboratories had been exposed to Brucella and that, although two Brucella isolates had been handled by both laboratories, infections in the two microbiologists were caused by two unrelated isolates. Because Brucella spp. pose a risk for aerosol-transmitted infection, CDC recommended risk assessment for all Brucella-exposed laboratory workers, postexposure prophylaxis (PEP) for those at high risk, surveillance for symptoms of disease, and serologic follow-up with workers. The events in Indiana and Minnesota emphasize the importance of adhering to recommended biosafety practices, timely sharing of information regarding laboratory exposures, and rapid implementation of response protocols. Case ReportsIndiana. On September 28, 2006, a microbiologist aged 47 years (microbiologist A) who worked at a clinical laboratory had onset of high fever, sweating, malaise, anorexia, headache, and hip pain. Initially, her symptoms were not severe; she did not seek medical treatment until 3 weeks later, after her symptoms had progressively worsened. The microbiologist was hospitalized on October 22 and recovered fully with treatment. On October 26, an unidentified blood culture isolate from microbiologist A (isolate A) was submitted for identification to a Minnesota clinical laboratory and determined to be Brucella spp.; both MDH and IDSH were notified of the finding. Epidemiologic investigation later revealed that, on July 17, microbiologist A had subcultured on an open laboratory bench an unidentified isolate (isolate C) from a referring laboratory. Isolate C subsequently was forwarded for identification to the same Minnesota clinical laboratory and identified as Brucella spp. Minnesota. On October 25, a microbiologist aged 61 years (microbiologist B), who worked at the same Minnesota clinical laboratory that received microbiologist A's isolate, had onset of low-grade fever, fatigue, and night sweats. She was hospitalized and recovered with treatment. On November 9, the Minnesota laboratory identified a blood culture isolate from microbiologist B (isolate B) as Brucella spp. and notified MDH. The subsequent investigation determined that microbiologist B had not handled isolate A from microbiologist A. However, previously she had handled on an open bench two unidentified isolates subsequently identified as Brucella spp. Her first exposure had occurred on July 21 while she was handling isolate C, which had been forwarded from the Indiana clinical laboratory. The second exposure had occurred on August 8 during testing of an isolate from a Texas referring clinical laboratory (isolate D). Investigation and ResponseThe investigation revealed that all potentially implicated specimens or isolates had been manipulated on an open bench, the routine practice for handling unidentified isolates in these laboratories. No spills or aerosol-generating procedures had occurred. Neither laboratory had formal protocols for 1) notification and follow-up of staff members who worked with isolates identified as Brucella spp. or 2) notification of laboratories that forwarded isolates later identified as Brucella spp. Brucella-exposed workers* from each laboratory were identified, and their exposures were classified as either high risk or low risk.† In Indiana, 105 staff members were exposed; 15 of those exposures were classified as high risk, including the exposure of microbiologist A. In Minnesota, 41 staff members were exposed; 13 of those exposures were classified as high risk, including the exposure of microbiologist B. All staff members classified with high-risk exposure, other than the two microbiologists who received antimicrobial therapy, were advised to receive PEP. To determine the source of the Brucella infections, CDC compared blood culture isolates from the two microbiologists with the isolates they handled, using multiple-locus variable number tandem repeats analysis at 21 genomic regions. All isolates were identified as Brucella melitensis biovar 3. Matching of 16 genomic amplicons suggested that isolate C was the source of infection for microbiologist A, the Indiana microbiologist. Matching of 17 genomic amplicons suggested that isolate D was the source of infection for microbiologist B, the Minnesota microbiologist. Serial serum samples from the 105 exposed Indiana laboratory staff members, excluding microbiologist A, were tested at CDC for anti-Brucella antibodies, using the Brucella microagglutination test (BMAT); the Minnesota laboratory conducted voluntary serial BMAT testing for 11 exposed laboratory staff members. No additional infections were detected in either group. Reported by: J Griffith, MPH, M Sullivan, MPH, Minnesota Dept of Health. J Howell, DVM, Indiana State Dept of Health. Div of Foodborne, Bacterial, and Mycotic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; EIS officers, CDC. Editorial Note:Brucellosis is a bacterial zoonotic infection usually caused by Brucella abortus, B. melitensis, Brucella suis, or less commonly by Brucella canis. Humans usually are infected by occupational exposure to infected animals, consumption of unpasteurized dairy products from infected animals, or inhalation of infectious aerosols. The average incubation period for brucellosis is 2--10 weeks but ranges from a few days to 6 months. Symptoms include intermittent fever, chills, malaise, sweating, joint and lower back pain, headache, anorexia, and fatigue (1). Untreated brucellosis can last from several weeks to several years. Chronic untreated brucellosis can lead to abscesses in the liver, spleen, heart valves, brain, or bone; osteoarticular complications; and, in rare cases, death. A definitive diagnosis requires that bacteria be cultured from clinical specimens. A presumptive diagnosis requires demonstrating high or rising titers of specific antibodies in the serum (1). Since 1986, fewer than 150 cases of brucellosis have been reported annually in the United States (2; CDC, unpublished data, 2007). However, brucellosis is among the most commonly reported laboratory-acquired bacterial infections (3). In a review of laboratory-associated infections during 1979--1999, Brucella spp. accounted for approximately 8% of all laboratory infections, 16% of bacterial infections, and 4% of deaths (4). Infections have occurred from sniffing culture plates, spilling blood-culture bottles, mucocutaneous exposure to sprays of organism-containing suspensions, aerosol generation from ruptured centrifuge tubes, or routine laboratory work with Brucella cultures outside of biological safety cabinets (5--9). Biosafety level 3 (BSL-3) practices, containment equipment, and facilities are recommended for all manipulations of Brucella cultures (Box 1) (10). Because unidentified isolates are commonly manipulated on an open bench, inadvertent exposure can occur when Brucella unexpectedly grows in a culture. A formal notification and response protocol must be used after identification of Brucella spp. Timely identification, notification, and appropriate follow-up of potentially exposed workers, in combination with worker training to maximize awareness and observance of appropriate safety practices, can prevent unnecessary illness and hospitalization from brucellosis. Exposures can be minimized by clinicians and forwarding laboratories clearly identifying specimens they suspect to be Brucella. Once Brucella has been identified (or is highly suspect), clinical laboratories should notify the state health department and send the isolate to the state public health laboratory or nearest Laboratory Reference Network laboratory for confirmation and species identification. When Brucella is confirmed, the state public health laboratory should notify all other laboratories that handled the specimen, and exposure to workers should be assessed at the submitting laboratory and other laboratories involved. Classification of exposures as high risk or low risk by practitioners of occupational health, infection control, or public health determines PEP recommendations. PEP is recommended for persons with high-risk exposure (Box 2). Serologic follow-up for exposed persons using quantitative assays (e.g., BMAT) should be performed at the time of exposure and at weeks 2, 4, 6, and 24 after exposure. Active, regular (e.g., weekly) surveillance for symptoms consistent with brucellosis should be conducted for all exposed laboratory workers for 6 months after exposure. PEP and monitoring differ for persons exposed to B. abortus RB51, an attenuated veterinary vaccine strain that is less commonly associated with human illness, is rifampin resistant in vitro, and does not elicit a measurable serologic response using available tests (Box 2). Laboratory workers who might have been exposed to Brucella and who have unexplained febrile illness consistent with brucellosis should be referred to health-care providers for evaluation. Evaluation should include blood culture and anti-Brucella antibody serologic testing, and treatment for brucellosis should be initiated when compatible illness is confirmed. Brucella spp. are dangerous infectious bacteria listed among CDC's category B bioterrorism agents.§ CDC and the Animal and Plant Health Inspection Service (APHIS) regulate the transfer, possession, or use of such agents in the United States. New isolations, laboratory exposures, and other incidents associated with the intentional or unintentional release of B. abortus (excluding RB51), B. melitensis, or B. suis must be reported as soon as possible to either CDC or APHIS.¶ Persons seeking assistance in identifying Brucella spp. or serologic monitoring of exposed persons should contact their state health departments or the CDC Bacterial Zoonoses Branch at telephone, 404-639-1711. References
* A Brucella-exposed worker was defined as any person present in the microbiology laboratory from the time the culture was first manipulated until all culture isolates were destroyed or removed from the laboratory. † A high-risk exposure was defined as 1) having direct personal exposure (e.g., sniffing bacteriologic cultures; direct skin contact; pipetting by mouth; inoculation; or spraying into the eyes, nose, or mouth), 2) performing work on an open bench (i.e., outside of biosafety level 3 containment equipment) with an open culture plate containing a Brucella isolate or being in close proximity to such work (e.g., across an open bench top or within 5 feet), or 3) presence in the laboratory during any procedure conducted on a Brucella isolate that might result in generation of aerosolized organisms and inhalational exposure (e.g., vortexing or catalase testing). A low-risk exposure was defined as being present in the laboratory during an exposure but not meeting the definition for a high-risk exposure. § Available at http://www.bt.cdc.gov/agent/agentlist-category.asp. ¶ Instructions for reporting are available at http://www.selectagents.gov.
Box 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 1/16/2008 |
|||||||||
|