|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
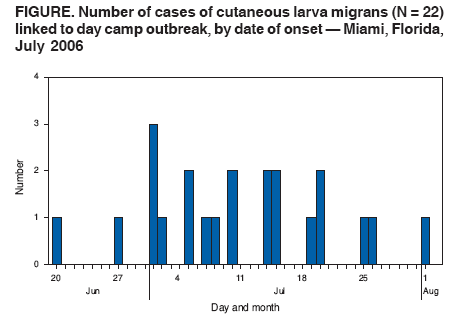
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Cutaneous Larva Migrans at a Children's Camp --- Miami, Florida, 2006On July 19, 2006, the director of a children's aquatic sports day camp notified the Miami--Dade County Health Department (MDCHD) of three campers who had received a diagnosis of cutaneous larva migrans (CLM), or "creeping eruption," a skin condition typically caused by dog or cat hookworm larvae of the genus Ancylostoma (1). MDCHD conducted an investigation to determine the source and magnitude of the outbreak and prevent additional illness. This report summarizes the results of that investigation, which identified exposure to cat feces in a playground sandbox as the likely source of infection. Although CLM outbreaks are reported rarely to the Florida Department of Health, evidence indicates that CLM is a potential health hazard in Florida (2). This disease cluster highlights the importance of appropriate environmental hygiene practices and education in preventing CLM. The camp property, which is located in Miami, includes swimming pools and a main building, volleyball court, playground with a sandbox, picnic area, and beach for boating and swimming. The camp consisted of four, 2-week sessions held during June 5--July 28, 2006, and was divided into two programs: a half-day session for children aged 2--6 years, and a full-day session for children aged 5--15 years. Approximately 300 campers and 80 staff members attended each session. On July 20, camp administrators announced to all current campers, their parents, and staff members that three children had received CLM diagnoses. Parents were asked to look for various symptoms of infection, including a snake-shaped (serpiginous) red rash, itching, and pus-containing lesions. In addition, camp administrators provided information about CLM to the households of any other campers and staff members who attended sessions during the summer. MDCHD advised that persons with signs or symptoms seek medical care and contact the health department to make a report. MDCHD received a total of 22 reports of persons (four staff members and 18 campers, including the three initial patients) with signs or symptoms of CLM. To identify cases, MDCHD staff members conducted telephone interviews of these persons by using a 60-item questionnaire that collected information regarding demographic variables, illness history, and activity history. A case was defined as illness consistent with CLM in a staff member or camper who attended the camp at any time during June 5--July 20, 2006, and had symptoms during June 5--August 20. All 22 persons who reported signs or symptoms met the case definition. Although no laboratory samples were obtained, all 22 patients had received a clinical diagnosis of CLM. MDCHD conducted a descriptive, cross-sectional study of the 22 cases and an environmental health assessment of the camp property. Illness onset occurred during June 20--August 1 (Figure). The median age of campers was 4 years (range: 2--6 years); median age of staff members was 17 years (range: 16--19 years). Patients had signs and symptoms including erythema (100%), pruritic rashes (100%), serpiginous lesions (77.3%), changing location of rash or lesions (50.0%), blistering lesions (27.3%), and pus-containing lesions (18.2%). Lesions were noted on the buttocks (68.2%), feet (45.5%), legs (27.3%), hands (9.1%), groin (9.1%), and abdomen (4.5%). Nine (40.9%) of the patients had lesions in more than one location either during a single episode or during the course of the infection. All but two patients used a nonprescription topical ointment at home before seeking medical attention, and all 22 patients sought medical attention. MDCHD contacted every physician to confirm CLM diagnoses. Patients were treated with thiabendazole, mebendazole, albendazole, or ivermectin. The mean length of time patients were at the camp was 3.7 weeks. Approximately 40.9% attended for 2 weeks, and 27.3% attended for >6 weeks. At the time interviews were conducted (July 19--September 2), six (27.3%) of the 22 patients were still attending the camp, and 18 (81.8%) were still experiencing symptoms. All 22 patients participated in the half-day camp for children aged 2--6 years. Although campers and staff members for both the half-day and full-day camps were exposed to sand from the beach and the volleyball court, only those in the half-day camp were allowed in the playground area, which included a sandbox containing approximately 400 cubic feet of sand that had been placed in the box 2 years previously. Campers were in or around the sandbox for approximately 1 hour each day, and all campers wore bathing suits while in this area. Fourteen (63.7%) of the 22 who became ill did not wear shoes while sitting in the sandbox. Four (18.2%) of the persons reported seeing cats near the sandbox. MDCHD investigators arrived at the site on July 19 to investigate the camp grounds and interview camp administrators. Camp administrators had sectioned off the sandbox already to prevent children from using the area; the camp director had researched CLM online and identified contaminated sandboxes as possible sources of infection. During their initial visit to the site, MDCHD investigators observed cats around the playground sandbox and noticed animal feces inside the sandbox; no fecal samples were collected. Interviews with the camp director revealed that general beach areas, to which all campers in both age groups were exposed, were frequented by dogs; therefore, the sand in general beach areas also was considered a possible source of exposure. Additional possible sources of exposure considered included 1) having pets at home (10 patients [45%]; eight dogs, one cat, one unknown); 2) being exposed to another nearby beach in the week before symptom onset (nine [41%]); and 3) sharing personal items such as towels or clothes with other campers (four [18%]). After analyzing initial data collected during July 19--25, MDCHD suspected that the sandbox was the source of infection. Staff members inspected the camp again on July 26 and did not find feces in the sandbox for laboratory testing. Immediately after the July 26 inspection, sand in the sandbox was removed and replaced. Two feral cats were removed from the premises by animal control and euthanized; the cats were not tested for hookworm. MDCHD staff recommended to camp administrators that the sandbox be covered with a tarp when not in use to prevent fecal contamination and to change the sand regularly in accordance with American Academy of Pediatrics and American Public Health Association standards (3). Administrators also were advised to report stray animals to animal control for removal and to inspect the sandbox daily and remove feces to reduce the number of potentially infective larvae; larvae typically do not emerge from their eggs in <24 hours. After the interventions were implemented on July 26, three additional cases were reported through September 2; however, these persons might have been exposed before the interventions were in place. Reported by: E O'Connell, MPH, J Suarez, F Leguen, MD, G Zhang, MD, M Etienne, A Torrecilla, A Jimenez, MPH, F Farahi, MPH, M Alzugaray, D Rodriguez, MPH, Miami--Dade County Health Dept; S Pizano, DVM, Miami--Dade County Animal Svcs; C Blackmore, DVM, PhD, D Goodman, PhD, RS Hopkins, MD, P Ragan, PhD, Florida Dept of Health. J Schulte, DO, T Doyle, MPH, CDC. Editorial Note:CLM is caused by dermal contact with sand or soil contaminated with eggs that are shed in the feces of hookworm-infected animals. In a study of feral cats in Florida, 75% were infected with Ancylostoma tubaeforme, and 33% were infected with Ancylostoma braziliense (2); A. braziliense is the species most commonly associated with CLM in humans (4). Although no stool samples were obtained from the cats in this study, the sandbox was considered the likely source of infection because only campers and staff members who were exposed to the sandbox were infected, and cat feces were observed in that area. In addition, each morning before camp, staff members raked the sand, burying any visible feces, which likely spread fecal matter throughout the sandbox. CLM outbreaks are more common in tropical or subtropical climates (5). Risk factors include contact with warm, moist, sandy soil and travel to an area where the disease is endemic (6). The larvae cannot complete their life cycle in a human host because they cannot penetrate the epidermal membrane of the skin; therefore, cutaneous infections usually resolve spontaneously within weeks or months, although disease duration as long as 55 weeks has been reported. Complications can include secondary bacterial infections, Löffler syndrome, and eosinophilic enteritis (1). In addition, pregnant women and children are at risk for complications from hookworm anemia.* CLM diagnosis usually is based on physical examination and activity history. Effective treatment is primarily with antihelminthic agents; other treatments include nitrogen cryotherapy. Orally administered albendazole or ivermectin or topically administered thiabendazole are the recommended therapies (7). However, both treatments can have side effects, such as nausea, diarrhea, anorexia, dizziness, headache, swelling of lymph nodes, and allergic reactions; safety of these drugs during pregnancy has not been established (8), placing increased importance on prevention (9). Hookworm treatment for cats and dogs is the primary means for preventing CLM. Pet owners should take their animals to a veterinarian to be tested and treated for hookworms on a biannual or yearly basis (10). In addition, stray animals should be reported to animal control, and animal feces should be removed promptly from areas of human activity (2). References
* Additional information available at http://www.cdc.gov/ncidod/dpd/parasites/hookworm/factsht_hookworm.htm and http://www.cdc.gov/ncidod/dpd/women.htm.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 12/12/2007 |
|||||||||
|