|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
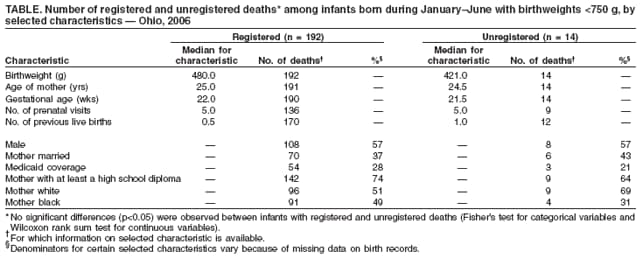
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Unregistered Deaths Among Extremely Low Birthweight Infants --- Ohio, 2006In the United States, infants with birthweights <750 g (i.e., extremely low birthweight infants) account for <1% of all births but approximately one third of the total infant mortality rate (1). Because these infants often have short life spans, their deaths might be misclassified as fetal deaths, leading to an underestimation of the overall infant mortality rate. Accurate infant mortality rates are important for program planning and evaluation, identification of health disparities and emerging trends, and development of prevention strategies. To assess the extent of unregistered deaths among extremely low birthweight infants born in Ohio during January--June 2006, the Ohio Department of Health analyzed birth and death records from this period for all infants with birthweights <750 g (1.7 lbs) and contacted birth hospitals to follow up on the discharge status of these infants. This report describes the results of that analysis, which indicated that 7% of the extremely low birthweight infants who were born in Ohio during this period, and who subsequently died, had deaths that were unregistered. The findings emphasize the need for routine verification of the discharge status of these infants from their birth hospitals and follow-up to ensure proper registration of deaths. Birth records for all infants with birthweights <750 g born in Ohio during January 1--June 30, 2006, were identified and matched with death records registered through December 31, 2006, using the Ohio Department of Health's vital statistics database. The birth hospitals of infants with only birth records were contacted by telephone to verify discharge status (i.e., alive to home, alive transferred, or deceased). Deaths among infants that were confirmed (via medical-record review) by the birth hospitals but for which no death records were found were considered unregistered deaths. Selected characteristics of extremely low birthweight infants with unregistered deaths (e.g., birthweight, race, and Medicaid coverage) were compared with those with registered deaths using data from birth records. Categorical variables were analyzed using Fisher's exact test, and continuous variables were analyzed using the Wilcoxon rank sum test. Among the 325 infants with birthweights <750 g, 192 (59%) had registered deaths, and 129 (40%) had no death records on file. Of the 129 infants with no death records on file, 115 (89%) were confirmed to be alive at the time of discharge from their birth hospitals; 14 (11%) were confirmed by their birth hospitals to have died. Thus, among the 325 extremely low birthweight infants, 206 deaths occurred, of which 192 (93%) were registered and 14 (7%) were unregistered. No statistically significant (p<0.05) differences were observed when comparing infants with unregistered deaths to those with registered deaths (Table). Reported by: J Paulson, MS, W Ramsini, PhD, Ohio Dept of Health. E Conrey, PhD, R Duffy, DDS, National Center for Chronic Disease Prevention and Health Promotion; MP Cooper, MD, EIS Officer, CDC. Editorial Note:Deaths among infants with extremely low birthweights are more likely to be unregistered because of the often short life spans of these infants and the potential for their deaths to be misclassified as fetal deaths. Previous studies indicate that numerous infant deaths likely have not been registered (2--4). In addition, in 2006, an analysis of CDC's linked birth/infant death data set for 2002--2004 demonstrated that numerous states reported infant mortality rates for infants with birthweights <500 g that were implausibly low (CDC, unpublished data, 2006), leading to concerns that these deaths were not being registered. CDC recognizes that deaths among low birthweight infants might not be registered and requires that all states follow up on the discharge status of infants with birthweights <750 g. However, not all states currently supply this information to CDC, and the number of deaths that are not registered in many states remains unknown. These practices might indicate that states are underestimating their infant mortality rates, leading to an overall underestimation of the national infant mortality rate, information that is important to agencies for policy planning, program evaluation, research, and identification of health disparities and trends. The results of this analysis indicate that an estimated 7% of deaths among infants born in Ohio with extremely low birthweights are not being registered. Reasons for the lack of registration of these deaths likely include confusion regarding whether they were fetal deaths or deaths of live-born infants. Although the resulting adjustment to Ohio's overall infant mortality rate is not substantial, programs that rely on accurate birthweight-specific infant mortality rates likely will observe a more pronounced effect. As a result of these findings, in 2007, the Ohio Department of Health plans to implement routine follow-up of infants with birthweights <750 g to ensure accurate birth and death records. This follow-up will include routine verification of the discharge status of all infants with birthweights <750 g and will ensure that all deceased infants have a registered death certificate. Officials in states that are not performing this follow-up also should consider implementing routine follow-up so that infant mortality rates are accurately reported. The findings in this report are subject to at least three limitations. First, the analysis was restricted to births that occurred in the first half of 2006. Findings from that period might not reflect the registration of deaths for the entire year. Moreover, a longer study period might have allowed for identification of any seasonal trends in registrations. Second, the small sample size might have prevented this analysis from detecting statistically significant differences between the registered and unregistered groups. Previous studies have indicated that the lack of registration of deaths in extremely low birthweight infants has occurred disproportionately for black infants, those born to unmarried mothers, and those born to mothers living in rural areas (2,3). Finally, the study design did not allow for identification of live-born infants whose deaths were misclassified as fetal deaths. Such infants would have received fetal death certificates instead of standard birth or death certificates. In addition to routine follow-up of infants with extremely low birthweights, further research regarding the reasons for the lack of registration of certain infant deaths is needed. Findings from such research might help in targeting interventions to improve the accuracy of infant death reporting. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/25/2007
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|