|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
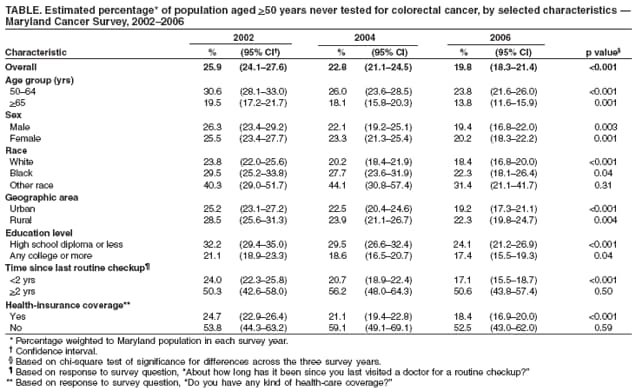
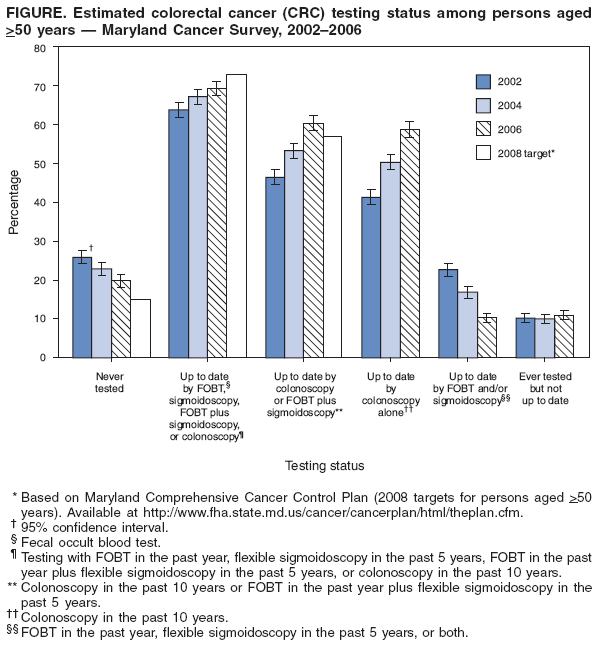
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Colorectal Cancer Test Use --- Maryland, 2002--2006During 2000--2004, Maryland had the thirteenth highest mortality rate for colorectal cancer (CRC) among the 50 states and the District of Columbia (1). The American Cancer Society (ACS), the U.S. Preventive Services Task Force, and other organizations recommend that adults begin CRC screening at age 50 years if they are at average risk for CRC and before age 50 years if they are at increased risk (2,3). For those at average risk, ACS recommends screening with 1) a fecal occult blood test (FOBT) or fecal immunochemical test (FIT) every year, 2) flexible sigmoidoscopy every 5 years, 3) an annual FOBT or FIT combined with flexible sigmoidoscopy every 5 years,* 4) double-contrast barium enema (DCBE) every 5 years, or 5) colonoscopy every 10 years (2). In 2002, the Maryland Department of Health and Mental Hygiene initiated the Maryland Cancer Survey (MCS) to assess testing prevalence and risk behaviors for seven types of cancer, including CRC. Reducing CRC mortality and disparities in CRC incidence and mortality are goals described in Maryland's Comprehensive Cancer Control Plan (MCCCP) (4). As milestones toward these goals, Maryland set the following targets for 2008 for persons aged >50 years: 1) decrease the percentage of Maryland residents who have never been screened for CRC to <15% (from a 2002 baseline of 25.9%); 2) increase the percentage of residents who are up to date with CRC screening (per ACS guidelines) to >73% (from a 2002 baseline of 63.8%); and 3) increase the percentage of residents who have been screened with either colonoscopy in the past 10 years, or FOBT in the past year plus flexible sigmoidoscopy in the past 5 years, to >57% (from a baseline of 46.5% in 2002). This report describes trends in CRC test use based on results from MCS surveys completed in 2002, 2004, and 2006.† The results indicated a significant decline (6.1 percentage points) in the percentage of Maryland residents aged >50 years who had never been tested for CRC, a 5.4 percentage-point increase in prevalence of up-to-date testing by any method, and a 13.9 percentage-point increase in prevalence of either colonoscopy in the past 10 years or FOBT in the past year plus flexible sigmoidoscopy in the past 5 years. However, Maryland residents who were neither white nor black (i.e., persons of other races) had a significantly lower prevalence of ever having a CRC test, as did persons without health insurance or those without a recent checkup. Although overall increases in CRC testing reflect substantial progress in Maryland, additional measures are needed to increase CRC testing among racial minority groups and the medically underserved. MCS is a biennial, population-based, statewide survey of cancer test use and behavioral risk factors among Maryland residents. MCS follows the methodology of the Behavioral Risk Factor Surveillance System (BRFSS) but focuses on adults aged >40 years, the population most at risk for cancer.§ The survey is conducted by telephone using random-digit dialing with computer-assisted telephone interviewing and list-assisted, disproportionate, stratified sampling. Respondents were eligible to participate in the survey if they were aged >40 years, resided in a private residence in Maryland, and were able to respond to the interview questions. For the purposes of sampling, Maryland was divided into two geographic strata, urban and rural, with oversampling of rural telephone numbers. In 2002 and 2004, the survey was offered only in English. In 2006, participants were able to respond in English or Spanish. Reported prevalence data were weighted to the Maryland population in the corresponding year according to BRFSS protocol (5). A total of 5,040, 5,004, and 5,149 persons completed the interviews in 2002, 2004, and 2006, respectively. Council of American Survey Research Organizations (CASRO) response rates were 38.4% (2002), 38.3% (2004), and 39.7% (2006). Of those persons surveyed in 2002, 2004, and 2006, a total of 3,436, 3,556, and 3,776 respondents, respectively, were aged >50 years. Respondents first were asked whether they had ever used a home FOBT or blood stool test and how long it had been since the last home test. After hearing a description of sigmoidoscopy and colonoscopy, respondents were asked whether they had ever had either test, which one was the most recent, and how long it had been since the last test. Questions regarding DCBE were not included in the questionnaire because DCBE is not commonly used as a first-line CRC screening test. Persons were considered to have up-to-date CRC testing if they reported any one of the following: an FOBT within the past year, a sigmoidoscopy within the past 5 years, an FOBT in the past year combined with a sigmoidoscopy in the past 5 years, or a colonoscopy within the past 10 years. Respondents whose responses were outside these parameters were considered not up to date, as were those who did not know when their last test occurred (6.8% of persons categorized as not up to date). The analysis is based on respondents aged >50 years who were able to report whether they had received any CRC tests and were able to distinguish whether their last lower gastrointestinal (GI) endoscopy was a sigmoidoscopy or colonoscopy (3,400 in 2002, 3,506 in 2004, and 3,748 in 2006; 99% of respondents aged >50 years for each year).¶ The estimated percentage of adults aged >50 years who had never had a CRC test decreased from 25.9% in 2002 to 19.8% in 2006, a decline of 6.1 percentage points (Figure). The percentage of respondents who were up to date with CRC testing by ACS guidelines increased by 5.4 percentage points during the study period, from 63.8% in 2002 to 69.2% in 2006. On the basis of 2006 MCS data, the percentage of Maryland residents who reported being up to date with colonoscopy or FOBT plus sigmoidoscopy has already exceeded the 2008 target of 57%. The prevalence of self-reported up-to-date colonoscopy (within the past 10 years) increased from 41.2% in 2002 to 58.7% in 2006. Accompanying the increase in colonoscopy during the study period was a decrease in the proportion of adults aged >50 years who were up to date by FOBT (within the past year) and sigmoidoscopy (in the past 5 years). The percentage of adults who were tested but were not up to date remained stable at 10.3%, 10.1%, and 11.0%, respectively, in the three survey years. The estimated percentage of Maryland residents never tested for CRC declined significantly (p<0.05, by chi-square test) during the study period by nearly all subject characteristics examined, except for respondents of other race (i.e., nonwhite and nonblack), those who had not had a routine checkup in the past 2 years, and those without health insurance coverage (Table). Persons with lower educational attainment (i.e., high school diploma or less) were significantly less likely to have ever been tested in each study year, but this disparity decreased over time. Persons who reported having a routine checkup within the past 2 years were more likely than those without a recent checkup to have ever been tested. Approximately 55% of the uninsured persons in each survey year had never been tested, compared with 24.7% (2002), 21.1% (2004), and 18.4% (2006) among persons with health insurance. Reported by: EK Steinberger, MD, CF Poppell, MS, M Zhan, PhD, F Shebl, MBBch, A Hopkins, MS, Univ of Maryland School of Medicine, Baltimore; C Groves, MSN, M Bienia, MBA, DM Dwyer, MD, Center for Cancer Surveillance and Control, Maryland Dept of Health and Mental Hygiene. Editorial Note:MCS results indicate that the percentage of Maryland residents aged >50 years who reported ever being tested for CRC increased by 6.1 percentage points from 2002 to 2006. Extrapolated to the state population aged >50 years (6), this finding translates into an estimated 90,000 previously untested Maryland residents who received CRC testing during that period. The observed prevalences in MCS of ever having any CRC tests are consistent with those reported in the Maryland BRFSS. The 2006 BRFSS indicated that 77.1% of Maryland residents aged >50 years had ever been tested for CRC, compared with 80.2% in the 2006 MCS. However, MCS, unlike BRFSS, asks respondents to specify which type of lower GI endoscopy was used in their most recent CRC test. Thus, MCS results have been able to highlight a trend toward increasing use of colonoscopy in recent years, with corresponding declines in testing with FOBT and sigmoidoscopy. The increase in CRC test use in general and colonoscopy in particular likely is attributable to recent changes in health-insurance coverage and to increased knowledge among the general public regarding CRC test procedures. Since July 2001, Medicare has provided payment for all types of CRC screening tests, including colonoscopy, which might account, in part, for the increase in testing among adults aged >65 years. Since 2001, the state of Maryland has required certain health-care insurers, health-maintenance organizations, and nonprofit health-services plans to provide CRC screening in accordance with ACS guidelines (7). In addition, since 2000, 23 of 24 Maryland jurisdictions have used funds from the Cigarette Restitution Fund Program to provide CRC education to health-care providers and the public or to provide CRC testing to qualified, low-income, uninsured residents (8). The MCS results also indicate that not all segments of the Maryland population have participated equally in these increases. Persons of other races (e.g., Asian, Native Hawaiian or other Pacific Islander, American Indian/Alaska Native, multiple race, and unspecified race), the medically underserved (i.e., those without health insurance), and persons without a routine checkup in the past 2 years have a substantially higher prevalence of never having had CRC testing. The findings in this report are subject to at least four limitations. First, findings from MCS are based on self-report and are not verified by medical chart review. Therefore, responses might be subject to social-desirability and recall bias. In addition, although the procedures of sigmoidoscopy and colonoscopy are described to survey respondents, certain respondents might not accurately identify their most recent test. Second, response rates in the MCS were low; however, they were comparable to those reported in the Maryland BRFSS (9). For survey years 2002--2006, CASRO rates ranged from 38.3% to 39.7% in the MCS and 36.8% to 44.0% in the Maryland BRFSS. The effect of nonresponse on survey estimates is difficult to determine because it depends on the extent to which nonrespondents differ from respondents and the general population. To reduce potential bias from nonresponse, interviewers made numerous call attempts and, when necessary, arranged appointments with respondents for more convenient times. Third, because MCS is a telephone survey, it excludes persons without landline telephones. The rates of cancer test use from telephone surveys might be overestimated because persons without landline telephones are less likely to have health insurance (10). Finally, the three survey samples consisted nearly entirely of English speakers. In 2002 and 2004, households that were reached by telephone but were unable to respond in English were excluded. However, in 2006, when the survey was offered in Spanish, only 0.4% of respondents chose to respond in Spanish. MCS elicits from respondents the specific type of lower GI endoscopy used in their most recent CRC test. Knowing whether the most recent endoscopy was a sigmoidoscopy or colonoscopy allows for better assessment of CRC testing practices. In Maryland, CRC testing rates have increased in recent years, with increases in up-to-date testing and a shift toward use of colonoscopy. Although these changes in CRC testing likely will have a substantial public health impact in Maryland (e.g., via the detection of premalignant lesions and early-stage CRC), additional measures are needed to eliminate remaining disparities in CRC testing and to increase testing among the medically underserved. References
* An annual FOBT or FIT combined with flexible sigmoidoscopy every 5 years is preferred over either of these options alone. † Results of 2002 and 2004 MCS surveys are available at http://fha.state.md.us/cancer/surveillance/html/data_reports.cfm. Results of the 2006 survey are in press. § MCS is conducted independently of the Maryland BRFSS. The Maryland BRFSS is available at http://www.fha.state.md.us/cphs/html/brfss.cfm. ¶ In this report, CRC tests performed for screening purposes are not differentiated from those performed for nonscreening reasons (e.g., diagnostic testing as follow-up to another test or because of symptoms). Therefore, the broader term "testing" is used in lieu of "screening" to reflect CRC tests performed for any indication.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/12/2007 |
|||||||||
|