|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
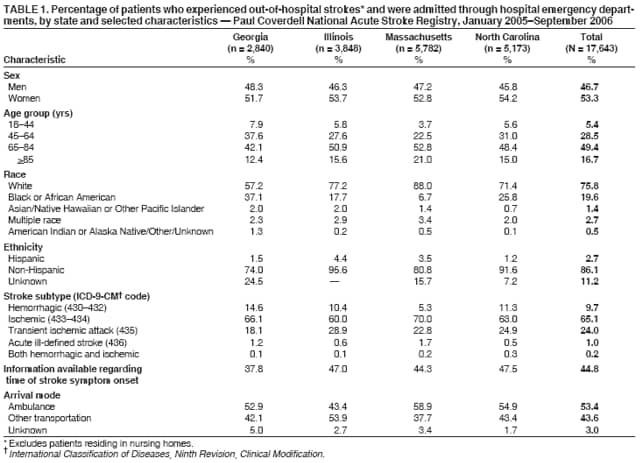
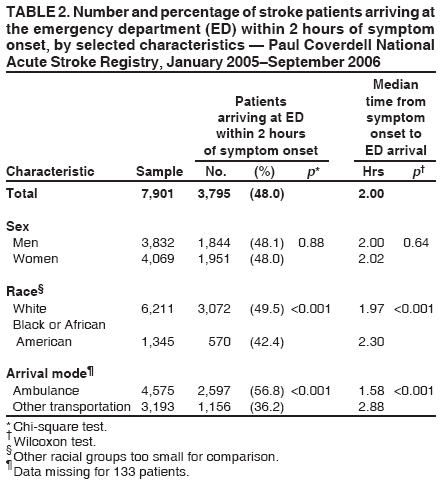
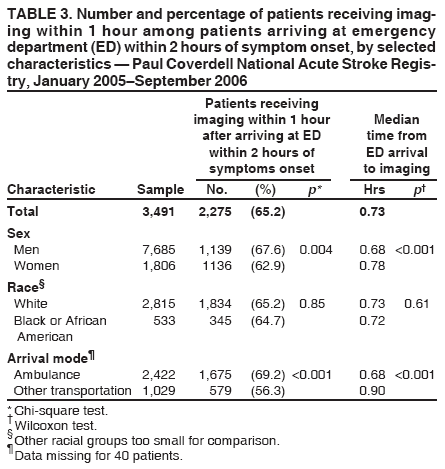
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prehospital and Hospital Delays After Stroke Onset --- United States, 2005--2006Each year approximately 700,000 persons in the United States have a new or recurrent stroke; of these persons, 15%_30% become permanently disabled, and 20% require institutionalization during the first 3 months after the stroke (1). The severity of stroke-related disability can be reduced if timely and appropriate treatment is received (2). Patients with ischemic stroke may be eligible for treatment with intravenous thrombolytic (i.e., tissue plasminogen activator [t-PA]) therapy within 3 hours of symptom onset (3). Receipt of this treatment usually requires patients to recognize stroke symptoms and receive prompt transport to a hospital emergency department (ED), where timely evaluation and brain imaging (i.e., computed tomography or magnetic resonance imaging) can take place. For patients eligible for t-PA, evidence suggests that the earlier patients are treated after the onset of symptoms the greater the likelihood of a more favorable outcome (4). In 2001, Congress established the Paul Coverdell National Acute Stroke Registry to measure and track the quality of care provided to acute stroke patients (5). To assess prehospital delays from onset of stroke symptoms to ED arrival and hospital delays from ED arrival to receipt of brain imaging, CDC analyzed data from the four states participating in the national stroke registry. The results of that analysis indicated that fewer than half (48.0%) of stroke patients for whom onset data were available arrived at the ED within 2 hours of symptom onset, and prehospital delays were shorter for persons transported to the ED by ambulance (i.e., emergency medical services) than for persons who did not receive ambulance transport. The interval between ED arrival and brain imaging also was significantly reduced for those arriving by ambulance. More extensive public education is needed regarding early recognition of stroke and the urgency of telephoning 9-1-1 to receive ambulance transport. Shortening prehospital and hospital delays will increase the proportion of ischemic stroke patients who are eligible to receive t-PA therapy and reduce their risk for severe disability from stroke. Data from the Paul Coverdell National Acute Stroke Registry were analyzed from the 142 hospitals participating in the four registry states (Georgia, Illinois, Massachusetts, and North Carolina). Hospital participation is voluntary, and each state has devised a process to select representative hospitals. Participating hospitals must collect data on all stroke patients admitted to the hospital during a collection period of at least 6 months of the year. Time of stroke symptom onset is based on patient and bystander information and is recorded in the registry. During January 1, 2005--September 30, 2006, these 142 hospitals collected data on 23,249 patients who experienced stroke or exhibited transient ischemic attack signs or symptoms defined by International Classification of Diseases, Ninth Revision, Clinical Modification discharge diagnosis codes 430--436. Excluded were patients who were institutionalized, resided in nursing homes, experienced strokes in the hospital, were not admitted to the hospital through its ED, or were hospital transfers, resulting in 17,643 patients for analysis. For this analysis, two temporal measures were used to reflect transport and brain imaging delays. Both are standard process measures used by the Coverdell registry. To reflect delays in transport, the proportion of patients who arrived at the ED within 2 hours of symptom onset was used. To reflect delays in imaging, the proportion of patients who received imaging within 1 hour of arrival in the ED among patients who arrived at the ED within 2 hours of symptom onset was used. These measures are derived from the 3-hour clinical window after symptom onset within which patients with ischemic stroke may be eligible for intravenous t-PA therapy. To enable comparison among groups, median times from symptom onset to ED arrival and from ED arrival to imaging also were calculated. The American Stroke Association has recommended a goal for patients to receive evaluation and a decision on treatment within 60 minutes of arrival in the ED (3). The significance of age-group differences by race and sex was analyzed using the t test. To determine whether racial disparities occurred in prehospital and hospital delays, white patients were compared with black or African American* patients; other racial/ethnic groups were too small in number for analysis. Mode of arrival at the ED was recorded as ambulance, nonambulance, and unknown. The chi-square test was used to examine the significance of differences in characteristics between patients arriving at the ED within 2 hours of symptom onset, compared with those arriving more than 2 hours after symptom onset. The chi-square test also was used to examine the differences in characteristics between patients receiving brain imaging within 1 hour of ED arrival compared with those who received imaging after 1 hour of arrival, among those patients who arrived in the ED within 2 hours of symptom onset. The Wilcoxon test was used to determine significance in differences in median times between groups; median times were restricted to <24 hours (6,7). Among the 17,643 patients in the study, 53.3% were women, 75.8% were white, 19.6% were black or African American, and 2.7% were Hispanic (Table 1). Overall, 66.1% of stroke patients were aged >65 years. Among these patients, women were older than men (mean age: 72.0 versus 67.7 years, p<0.001), and whites were older than blacks or African Americans (mean age: 72.2 versus 62.4 years, p<0.001). Ischemic stroke (65.1%) was the most common stroke subtype, followed by transient ischemic attack (24.0%) and hemorrhagic stroke (9.7%). More patients (53.4%) were transported by ambulance than by other means (43.6%) (Table 1). Information on the time of stroke symptom onset was recorded for 7,901 (44.8%) of the 17,643 patients. Among these patients, 3,795 (48.0%) arrived at the ED within 2 hours of stroke-symptom onset (Table 2). Significantly fewer blacks or African Americans (42.4%) arrived within 2 hours of symptom onset compared with whites (49.5%), and significantly fewer nonambulance patients (36.2%) arrived within 2 hours of symptom onset compared with patients transported by ambulance (56.8%) (Table 2). The median arrival time for all patients with known time of onset was 2.0 hours. Among the 3,795 patients who arrived at the ED within 2 hours of symptom onset, 3,491 had data recorded regarding the interval from ED arrival to receipt of brain imaging. A total of 2,275 (65.2%) received imaging within 1 hour of ED arrival. Significantly fewer women received imaging within 1 hour of ED arrival than men (62.9% versus 67.6%, p=0.004) (Table 3), and fewer nonambulance patients received imaging within 1 hour compared with patients transported by ambulance (56.3% versus 69.2%, p=0.001) (Table 3). No disparities among racial groups were observed regarding receipt of imaging within 1 hour of ED arrival (Table 3). Among those patients who arrived at the ED within 2 hours, the median time from ED arrival to brain imaging was 0.73 hours (43.8 minutes) (Table 3). Reported by: M Frankel, MD, Emory Univ, Atlanta, Georgia. J Hinchey, MD, Tufts_New England Medical Center; LH Schwamm, MD, Harvard Medical School, Boston; H Wall MPH, Massachusetts Dept of Public Health. KM Rose, PhD, Univ of North Carolina_Chapel Hill. MG George, MD, HF McGruder, PhD, A Liban, MPA, JB Croft, PhD, Div for Heart Disease and Stroke Prevention, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:For ischemic stroke patients to benefit from intravenous t-PA therapy, under current guidelines therapy should begin as soon as possible after diagnosis and determination of eligibility and within 3 hours of symptom onset (3). The findings described in this report indicate that fewer than half of the patients arrived at the ED within 2 hours of symptom onset, whereas nearly two-thirds of those who arrived at the ED within 2 hours of onset received brain imaging within 1 hour of ED arrival. The findings also indicate that a greater proportion of blacks or African Americans, compared with whites, had longer prehospital delay times. Previous studies have indicated mixed results as to whether race was related to prehospital delay (8). Further studies regarding the use of ambulances by stroke patients in minority populations are needed to determine culturally effective interventions to increase the use of ambulances. Patients arriving by ambulance had significantly shorter wait times for brain imaging. Consistent with previous reports (6), approximately half of the patients in the registry population arrived by ambulance. Arriving by ambulance might expedite triage decisions in the ED and lead to shorter delays before brain imaging. Both shorter prehospital and hospital delays will increase the proportion of patients with ischemic stroke who can receive brain imaging, t-PA therapy, and early secondary prevention therapies and reduce their risk for severe disability from stroke. Although some missing data might be attributed to record-keeping practices, the fact that time of symptom onset was recorded for only 44.8% of the stroke patients studied suggests a need for greater measures to educate the public to recognize the symptoms of stroke. Inability of patients to recognize stroke onset has been attributed to a lack of pain with symptoms and to cognitive, motor, and communication deficits (8). In some cases, stroke can even occur during sleep, without waking the patient. The Brain Attack Coalition (BAC) has proposed designation of certain hospitals as Primary Stroke Services (PSS) facilities that stabilize and provide emergency care for patients with acute stroke (9). BAC recommends that ambulance coordination with PSS EDs should be an integral component of services to ensure rapid evaluation and transport of acute stroke patients to appropriate facilities (10). Use of coordinated ambulance services that include advance notification to receiving hospitals can increase opportunities for receipt of t-PA among those with ischemic stroke (10). The findings in this report are subject to at least three limitations. First, time of symptom onset was recorded for fewer than half of the stroke patients. If delays experienced by patients with recorded onset were substantially different from those experienced by patients without recorded onset, selection bias might have resulted. In addition, this analysis did not differentiate between a time of onset when the patient or bystander first recognized stroke symptoms and a time when the patient was last known to be well before onset of symptoms. This difference might, in part, account for certain delays between onset of symptoms and arrival at the ED. Second, the results represent aggregate data from four states and are neither a random sample of stroke patients or hospitals from these states nor generalizable to other states; regional variations might be obscured, including differences in ambulance use by state. Finally, data were not weighted to reflect differences in hospitals, such as the number of stroke admissions, which might have led to underrepresentation of patients treated in smaller hospitals. To maximize the number of patients who are eligible to receive t-PA, further measures are needed to reduce prehospital delays. Specifically, additional actions are needed to increase the proportion of patients with acute stroke symptoms who are transported to EDs by ambulance (8), such as educating the public regarding the signs and symptoms of stroke and the importance of telephoning for ambulance transport. Hospitals are advised to continue to monitor and improve ED process times to reduce hospital delays before brain imaging for acute stroke patients. References
* The Coverdell registry uses the following racial categories in its data collection: white, black or African American, Asian, Native Hawaiian or Other Pacific Islander, American Indian or Alaska Native, other, specify (other), and unknown.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 5/17/2007 |
|||||||||
|