|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
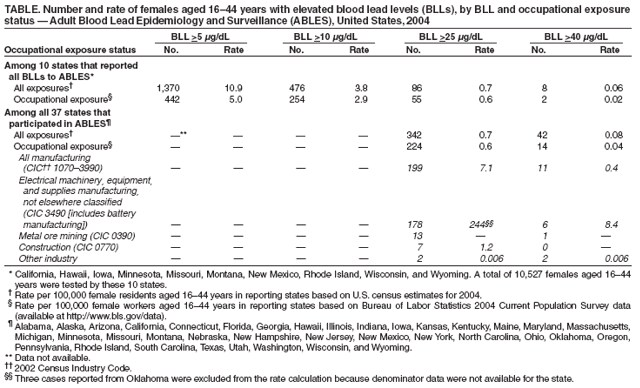
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Lead Exposure Among Females of Childbearing Age --- United States, 2004For centuries, exposure to high concentrations of lead has been known to pose health hazards, and evidence is mounting regarding adverse health effects from moderate- and low-level blood lead concentrations. Public health authorities use higher levels to define blood lead levels (BLLs) of concern in nonpregnant females (>25 µg/dL) compared with children (>10 µg/dL) and a lower level (>5 µg/dL) for pregnant females (1--3). This difference in levels for nonpregnant and pregnant females has raised concern because of the recognition that a proportion of nonpregnant females with BLLs >5 µg/dL will become pregnant and potentially expose their infants to a risk for adverse health effects from lead. Maternal and fetal BLLs are nearly identical because lead crosses the placenta unencumbered (4). This report summarizes 2004 surveillance data regarding elevated BLLs among females of childbearing age (i.e., aged 16--44 years) in 37 states participating in CDC's Adult Blood Lead Epidemiology and Surveillance (ABLES) program. The results indicated that rates of elevated BLLs ranged from 0.06 per 100,000 females of childbearing age at BLLs of >40 µg/dL to 10.9 per 100,000 females at BLLs of >5 µg/dL. Primary and secondary prevention of lead exposure among females of childbearing age is needed to avert neurobehavioral and cognitive deficits in their offspring. ABLES tracks laboratory-reported BLLs in persons aged >16 years who have been tested through workplace monitoring programs or on the basis of clinical suspicion of lead exposure; BLLs are reported for both occupational and nonoccupational exposures.* The Occupational Safety and Health Administration (OSHA) mandates BLL testing of all persons working in areas where airborne lead exceeds a certain level. States participating in ABLES require all laboratories to report BLL results. The lowest reportable BLL varies by state. During 2004, a total of 37 states participated in ABLES. These states all reported BLL rates of >25 µg/dL and >40 µg/dL. Ten of the 37 states also reported BLLs of any level, enabling these states to calculate prevalences of persons with BLLs >5 µg/dL and >10 µg/dL, in addition to the two higher levels. To assess the prevalence of elevated BLLs in females of childbearing age, ABLES data for 2004 were analyzed at four different BLLs: 1) 5 µg/dL, the level at or above which the Association of Occupational and Environmental Clinics recommends intervention for pregnant women (3); 2) 10 µg/dL, the level at or above which CDC recommends intervention for children (1); 3) 25 µg/dL, the limit set by Healthy People 2010 in its public health objective to eliminate elevated BLLs in adults (2); and 4) 40 µg/dL, the limit at or below which OSHA will permit a worker to return to work after being medically removed from work because of lead poisoning (5). Unique identifiers were used to exclude females who had multiple tests performed in 2004; for females with multiple tests, only the highest value was included. Occupationally exposed females were defined as those whose medical records contained either a valid industry code or a report of work-related exposure. Exposures lacking at least one of these two criteria were considered nonoccupational. Occupational denominators were based on the Bureau of Labor Statistics 2004 Current Population Survey (6). Rates of elevated BLLs resulting from all exposures (i.e., both occupational and nonoccupational) also were calculated per 100,000 female residents aged 16--44 years in the reporting states, using U.S. census population estimates for 2004 as the denominators. Using case data from all 37 ABLES states, rates of BLLs >25 µg/dL and BLLs >40 µg/dL among occupationally exposed females aged 16--44 years were calculated per 100,000 female workers aged 16--44 years overall and in individual industries with high numbers of workers with elevated BLLs. Using data from 10 ABLES states, rates also were calculated at BLLs of >5 µg/dL and >10 µg/dL. In 2004, in 10 ABLES states, a total of 10,527 females aged 16--44 years were tested, and all BLLs for this group were reported. Of the number tested, 1,370 (13.0%) had BLLs >5 µg/dL (10.9 per 100,000 female residents aged 16--44 years), and 476 had BLLs >10 µg/dL (3.8 per 100,000 female residents aged 16--44 years) (Table). A total of 442 (32.3%) of the 1,370 females with BLLs >5 µg/dL had occupational exposures. In all 37 ABLES states, the total number of females aged 16--44 years who were tested is unknown. Among those tested, 0.7 per 100,000 female residents aged 16--44 years had BLLs >25 µg/dL, and 0.08 per 100,000 female residents had BLLs >40 µg/dL (Table). The rates of elevated BLLs associated with occupational exposure were similar to or lower than the rates associated with all exposures (i.e., both occupational and nonoccupational) at all four levels examined; however, certain industry-specific rates of occupational exposure were substantially higher than all other rates (Table). The majority of occupationally exposed females were employed in the manufacturing sector, with 178 of 199 (89%) working in the industry that includes battery manufacturing (Table).† For that industry, these 178 females yielded a rate of 244 cases of BLLs >25 µg/dL per 100,000 females aged 16--44 years employed in the industry. This rate compares with rates of 7.1 cases of BLLs >25 µg/dL per 100,000 in the entire manufacturing sector and 0.6 cases per 100,000 employed in all sectors. Similarly, the industry that includes battery manufacturing had a rate of 8.4 cases of BLLs >40 µg/dL per 100,000 females aged 16--44 years employed in that industry, compared with rates of 0.4 per 100,000 employed in the entire manufacturing sector and 0.04 per 100,000 employed in all sectors (Table). Reported by: GM Calvert, MD, RJ Roscoe, MS, Div of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health; SE Luckhaupt, MD, EIS Officer, CDC. Editorial Note:Health effects in infants born to females with moderately elevated BLLs (i.e., 10--15 µg/dL) include preterm birth, decreased gestational maturity, lower birth weight, reduced postnatal growth, increased incidence of minor congenital anomalies, and early neurologic or neurobehavioral deficits (7). How long these neurologic effects are likely to persist is unclear, but some evidence documents associations between prenatal elevated BLLs and decreased intelligence at ages 3--7 years (8). Conducting surveillance of elevated BLLs among all females of childbearing age is important because approximately one third to one half of U.S. pregnancies are unplanned (9). Identification of a female with elevated BLLs can facilitate prevention of any further lead exposure that might, in the event she becomes pregnant, endanger the health of the fetus. Estimates of the number and rate of females of childbearing age with elevated BLLs have varied widely. Data from the National Health and Nutrition Examination Survey (NHANES) for 1999--2002 suggest a national rate of 300 cases of BLLs >10 µg/dL per 100,000 women aged 20--59 years, a 25% decrease from 1991--1994 NHANES estimates of 400 cases per 100,000 population. For comparison, in this report, data from the 10 states that reported all BLLs to ABLES in 2004 indicated a rate of only 3.8 cases of BLLs >10 µg/dL per 100,000 females aged 16--44 years for all types of exposures. Because the rates of BLLs >25 µg/dL and BLLs >40 µg/dL from the 10 states were similar to the rates derived from reports of all 37 ABLES states (Table), the ABLES data offer no indication that lead exposures in the 10 states would differ substantially from exposures in all 50 states combined. The data presented in this report, however, used the general population of female residents aged 16--44 years as the denominator. For the ABLES rate to approximate the rate from NHANES, all females in that population who met lead exposure criteria for workplace monitoring programs or who were suspected of lead exposure by health-care providers would have been tested and reported to ABLES. However, the low numbers (10,527) of females tested in the 10 states suggests this likely was not the case; using the NHANES rate, approximately 37,000 females aged 16--44 years in the 10 states would have had BLLs >10 µg/dL. The difference between the ABLES population-based rates and the rates from NHANES suggest that a large proportion of females with moderately elevated BLLs likely are not being tested or the results are not being reported to ABLES. Rates of elevated BLLs detected in ABLES among females in the manufacturing sector, especially in the industry that includes battery manufacturing, were much higher than rates among the general population for all lead exposures. These higher rates suggest that despite OSHA's recent focus on reducing workplace lead exposures among all U.S. workers, the workplace remains a substantial source of exposure, and clinicians should consider work history when determining whether to measure BLLs. The findings in this report are subject to at least three limitations. First, elevated BLLs are underreported by ABLES because all employers might not provide BLL testing to all lead-exposed workers as required by OSHA regulations, and testing of nonoccupationally exposed adults is dependent on a clinician's index of suspicion. Underreporting likely varies by industry. For example, high rates of elevated BLLs in the industry that includes battery manufacturing might partially reflect more thorough testing programs in this industry. In addition, certain laboratories might not report all tests as required by state regulations. Second, data on occupational sources of exposure might be incomplete, resulting in misclassification of occupational versus nonoccupational cases. Finally, a wide margin of error is associated with certain industry-specific rates because of the small sample size. The difference between BLLs that are considered elevated in females who are pregnant and those who might become pregnant has substantial public health implications. Identifying and counseling females of childbearing age who might become pregnant and expose children to lead in utero might help to prevent neurobehavioral and cognitive deficits. Acknowledgment This report is based, in part, on data contributed by ABLES state coordinators. References
* Additional information regarding the ABLES program is available at http://www.cdc.gov/niosh/topics/ables/ables.html. † 2002 Census Industry Code 3490.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/26/2007 |
|||||||||
|