|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
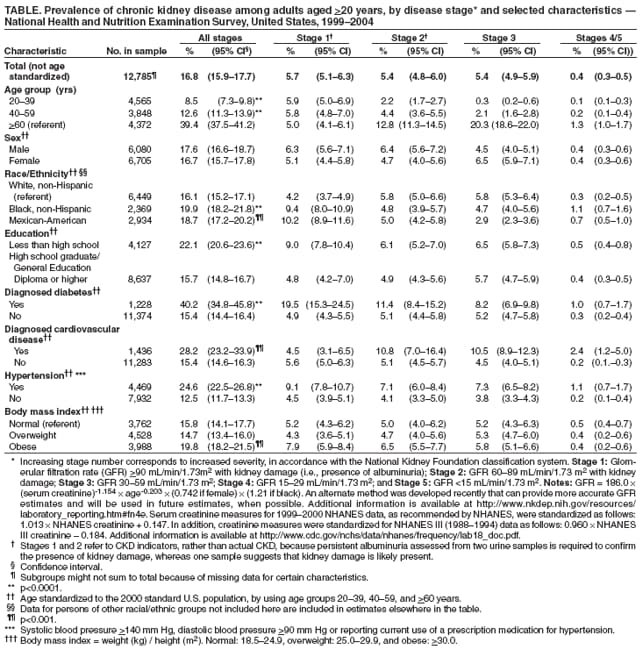
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Chronic Kidney Disease and Associated Risk Factors --- United States, 1999--2004Chronic kidney disease (CKD) is a serious condition associated with premature mortality, decreased quality of life, and increased health-care expenditures. Untreated CKD can result in end-stage renal disease and necessitate dialysis or kidney transplantation. Risk factors for CKD include cardiovascular disease, diabetes, hypertension, and obesity (1--3). To estimate the prevalence of CKD in the United States (overall and by health risk factors and other characteristics), CDC analyzed the most recent data from the National Health and Nutrition Examination Survey (NHANES). This report summarizes the results of that analysis, which determined that 16.8% of the U.S. population aged >20 years had CKD, according to 1999--2004 NHANES data, compared with 14.5% from the 1988--1994 NHANES (i.e., NHANES III), an increase of 15.9% based on crude estimates of prevalence* (4). Persons with diabetes or cardiovascular disease had a greater prevalence of CKD than persons without those conditions. The results underscore the need to continue surveillance for CKD and its risk factors in the United States and to implement new strategies to reduce the number of persons with this condition. NHANES is a continuous survey of the health and nutritional status of the U.S. civilian, noninstitutionalized population; samples of participants are selected through a complex, multistage probability design. NHANES collects data through interviews in participants' homes and medical examinations conducted in a mobile examination center.† Although data are collected continuously, they are released in 2-year increments. The analyses in this report use combined NHANES data from three survey periods: 1999--2000, 2001--2002, and 2003--2004. The NHANES examination includes measurement of serum creatinine and urine albumin and creatinine from a single spot urine test. For this study, kidney damage (stages 1 and 2 only) was suggested by the presence of albuminuria (i.e., abnormal amounts of urine albumin assessed by the urine albumin to urine creatinine ratio [ACR]).§ Persons with apparent kidney damage included those with microalbuminuria (ACR of 17--250 mg/g for men or 25--355 mg/g for women) or macroalbuminuria (ACR of >250 mg/g for men or >355 mg/g for women). Level of kidney function was estimated from the glomerular filtration rate (GFR), with lower values corresponding to diminished kidney function. CKD prevalence was estimated from apparent kidney damage and kidney function and categorized into stages, with increasing stage numbers corresponding to increased severity, according to the National Kidney Foundation classification system (2,5).¶ CKD prevalence estimates were calculated by demographic characteristics (i.e., age group, sex, race/ethnicity, and education level) and by CKD risk factors: diagnosed diabetes, diagnosed cardiovascular disease, hypertension,** and body mass index group.†† Diabetes was defined as self-report of diagnosis by a doctor or other health professional. Cardiovascular disease was defined as self-report of diagnosis by a doctor or other health professional of congestive heart failure, coronary heart disease, angina, stroke, or heart attack. Data were analyzed using sample weights to account for differential probabilities of sample selection, nonresponse, and sample noncoverage. Estimates by demographic characteristic and risk factor were age standardized to the 2000 U.S. standard population aged >20 years. Two sample t tests were used to test the statistical significance (p<0.05) of differences in CKD prevalence (all stages) between population subgroups. The total crude (i.e., not age-standardized) CKD prevalence estimate for adults aged >20 years in the United States was 16.8%. By disease stage, the prevalences were as follows: stage 1, 5.7%; stage 2, 5.4%; stage 3, 5.4%; stages 4/5, 0.4% (Table). By age group, CKD (all stages) was more prevalent among persons aged >60 years (39.4%) than among persons aged 40--59 years (12.6%) or 20--39 years (8.5%). By education level, CKD (all stages) was more prevalent among persons with less than a high school education (22.1%) than persons with at least a high school education (15.7%). CKD prevalence also was greater among persons with diabetes than among those without diabetes (40.2% versus 15.4%), among persons with cardiovascular disease than among those without cardiovascular disease (28.2% versus 15.4%), and among persons with hypertension than among those without hypertension (24.6% versus 12.5%). In addition, CKD prevalence was greater among non-Hispanic blacks (19.9%) and Mexican Americans (18.7%) than among non-Hispanic whites (16.1%). This racial/ethnic disparity was most pronounced among participants with stage 1 CKD. In that group, Mexican Americans had a prevalence of 10.2% and non-Hispanic blacks had a prevalence of 9.4%, compared with 4.2% for non-Hispanic whites. Reported by: S Saydah, PhD, M Eberhardt, PhD, National Center for Health Statistics; N Rios-Burrows, MPH, D Williams, MD, PhD, L Geiss, MA, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion; R Dorsey, PhD, EIS Officer, CDC. Editorial Note:This report provides the most current nationally representative estimates of CKD in the U.S. population. The findings indicate that CKD affected an estimated 16.8% of adults aged >20 years during 1999--2004, an increase from the recalculated NHANES III (1988--1994) estimate of 14.5%. Persons with CKD have high rates of morbidity, mortality, and health-care utilization (6,7). The findings in this report suggest that CKD is a growing health problem in the United States. CKD prevalence was greater among older persons and among persons with diabetes, cardiovascular disease, and hypertension than among persons without these conditions, supporting previous findings (2,6). Mexican Americans and non-Hispanic blacks had greater prevalence of CKD than non-Hispanic whites. The large disparity in prevalence among those with stage 1 CKD might be explained, in part, by racial/ethnic differences in microalbuminuria among non-Hispanic blacks and Mexican Americans (8). Activities aimed at preventing CKD or its progression can decrease prevalence of the most severe form of CKD, stage 5 (i.e., end-stage renal disease), which is associated with increased morbidity and mortality and diminished health-related quality of life (1). Both the incidence and prevalence of end-stage renal disease have increased during the past 30 years and are expected to continue increasing through 2010 (1,9). Treatments such as control of high blood pressure in the early stages of CKD can prevent progression to end-stage renal disease (2). The findings in this report are subject to at least four limitations. First, albuminuria was used to determine kidney damage for categorizing persons as having stage 1 and stage 2 CKD, but albuminuria is not the only marker for kidney damage. Urine sediment and abnormal imaging tests also are used to determine kidney damage; however, these tests were not available in NHANES. As a result, kidney damage and reported prevalence of stage 1 and stage 2 CKD might be underestimated (5). Second, estimates for stages 1 and 2 reflect CKD indicators, rather than actual disease, because two urine samples were not available in NHANES 1999--2004 to assess persistent albuminuria and confirm the presence of kidney damage. Previous analyses of NHANES III data demonstrated that using two urine tests to confirm kidney damage produced a lesser prevalence of stage 1 and stage 2 CKD compared with using one urine test, resulting in more conservative estimates for CKD overall (11.0% versus 14.5%). Thus, CKD in this report might be overestimated (4). Third, the data are cross-sectional, not longitudinal, preventing assessment of whether risk factors caused or resulted from CKD. Finally, the number of persons with stages 3, 4, and 5 CKD is small, limiting the power of the analysis and precluding separate estimates for persons with stage 4 and stage 5 and comparison of estimates by demographic characteristic and risk factor. New programs aimed at decreasing the number of CKD cases were established recently (1,10). The National Kidney Disease Education Program provides resources to the public, patients, and health-care professionals with the goal of reducing morbidity and mortality from kidney disease complications. World Kidney Day was instituted in 2006 to increase awareness of kidney disease and promote early detection. Continued surveillance of albuminuria and serum creatinine using NHANES can track the prevalence of CKD, monitor trends, and identify groups at high risk, enabling targeted programs. Finally, CDC is working with Johns Hopkins University and the University of Michigan to develop a comprehensive national surveillance system for CKD that will monitor early stages of the disease and its risk factors and the effects of CKD on the U.S. population. References
* To enable comparison of CKD prevalence from 1999--2004 NHANES with that from NHANES III (1988--1994), data from the older report were recalculated using 1999--2004 NHANES criteria, resulting in an estimated CKD prevalence of 14.5% for adults aged >20 years. The new criteria called for a single spot urine test to determine albuminuria (i.e., apparent kidney damage) instead of two tests (i.e., an initial test and a confirming test), which were conducted for some participants in NHANES III. For participants in NHANES III who had received two tests, the initial urine test was used in the recalculation. Initial analyses of NHANES data, using two tests, had resulted in an estimated CKD prevalence of 11.0% for adults aged >20 years. Comparison of crude estimates for CKD overall is presented because NHANES III data were not age standardized. † Additional NHANES information is available at http://www.cdc.gov/nchs/nhanes.htm. § Stages 1 and 2 refer to CKD indicators, rather than actual CKD, because persistent albuminuria assessed from two urine samples is required to confirm the presence of kidney damage, whereas one sample suggests that kidney damage is likely present. ¶ Stage 1: GFR >90 mL/min/1.73m2 with kidney damage (i.e., presence of albuminuria); Stage 2: GFR 60--89 mL/min/1.73 m2 with kidney damage; Stage 3: GFR 30--59 mL/min/1.73 m2; Stage 4: GFR 15--29 mL/min/1.73 m2; and Stage 5: GFR <15 mL/min/1.73 m2. Notes: GFR = 186.0 × (serum creatinine)-1.154 × age-0.203 × (0.742 if female) × (1.21 if black). An alternate method was developed recently that can provide more accurate GFR estimates and will be used in future estimates, when possible. Additional information is available at http://www.nkdep.nih.gov/resources/laboratory_reporting.htm#fn4e. Serum creatinine measures for 1999--2000 NHANES data, as recommended by NHANES, were standardized as follows: 1.013 × NHANES creatinine + 0.147. In addition, creatinine measures were standardized for NHANES III (1988--1994) data as follows: 0.960 × NHANES III creatinine -- 0.184. Additional information is available at http://www.cdc.gov/nchs/data/nhanes/frequency/lab18_doc.pdf. ** Systolic blood pressure >140 mm Hg, diastolic blood pressure >90 mm Hg, or reported current use of a prescription medication for hypertension. †† Body mass index = weight (kg) / height (m2). Normal = 18.5--24.9, overweight = 25.0--29.9, and obese = >30.0.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/1/2007 |
|||||||||
|