|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
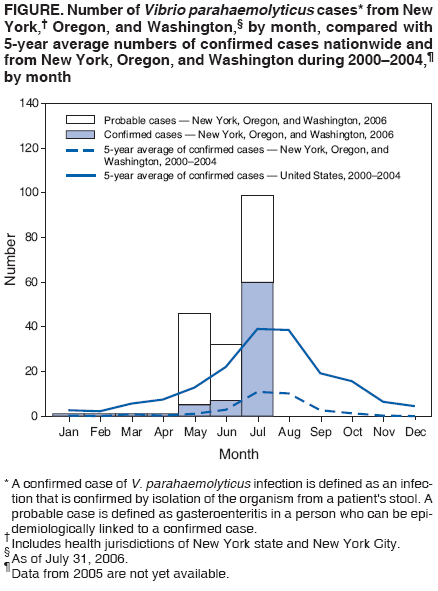
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Vibrio parahaemolyticus Infections Associated with Consumption of Raw Shellfish --- Three States, 2006On August 7, this report was posted as an MMWR Dispatch on the MMWR website (http://www.cdc.gov/mmwr). During May 20--July 31, 2006, New York City, New York state, Oregon, and Washington health departments reported a total of 177 cases of Vibrio parahaemolyticus infection, of which 122 have been associated with 17 clusters. A cluster has been defined as a group of two or more ill persons who were linked to the same shellfish source (e.g., shared a meal at the same restaurant or obtained shellfish from the same seafood market). Certain clusters were associated with restaurants, certain clusters with seafood markets, and certain clusters with recreational harvesting. Three patients were hospitalized; no fatalities have been reported. No demographic (e.g., age, sex, or race) or medical history (e.g., predisposing conditions) information is yet available regarding affected persons. A confirmed case of V. parahaemolyticus infection is defined as an infection confirmed by isolation of the organism from a patient's stool. A probable case is defined as gastroenteritis in a person who can be epidemiologically linked to a confirmed case. Of the 177 V. parahaemolyticus cases reported, 72 are confirmed and 105 are probable: New York City (two confirmed, 74 probable), New York state (seven confirmed), Oregon (eight confirmed, eight probable), and Washington (55 confirmed, 23 probable). This incidence of infection is much higher than expected; during May, June, and July 2000--2004, these jurisdictions reported an annual average of 16 laboratory-confirmed V. parahaemolyticus cases to CDC (Figure). The number of confirmed cases in this report (72) is more than the average number reported during May, June, and July during 2000--2004, in the entire United States (Figure). Subtyping of V. parahaemolyticus isolates has indicated that 18 of 23 isolates tested are serotype O4:K12, which is unrelated to the pandemic strain that was first identified in Asia in 1996 and later emerged in the United States in 1998 (1,2). Traceback investigations have linked contaminated oysters and contaminated clams to harvest areas in Washington and British Columbia, Canada; shellfish from these sources were distributed to seafood markets and restaurants nationwide. Ongoing investigations are being conducted by state and local health departments and regional Food and Drug Administration (FDA) shellfish-control offices to identify additional sources of infection. Additional infections likely have been undetected, underreported, or both. V. parahaemolyticus infection causes acute, self-limited gastroenteritis typically characterized by diarrhea, abdominal cramps, nausea, vomiting, fever, and chills of 1--3 days duration, with onset usually within 24 hours after eating contaminated food. Cases are most commonly reported during warmer months and are often associated with eating raw or undercooked shellfish or other cooked foods that have been cross-contaminated by raw shellfish. Previous local V. parahaemolyticus outbreaks have coincided with large increases in sporadic cases nationally, suggesting that identified clusters are most often manifestations of a wider increase in illness (1). Studies suggest that approximately 20 V. parahaemolyticus illnesses exist for each laboratory-confirmed case reported to CDC (3,4), underscoring the need for enhanced national surveillance and control measures. Shellfish harvest areas in the United States and Canada that were previously implicated in V. parahaemolyticus outbreaks are routinely monitored by state shellfish-control agencies to control transmission of these illnesses. Despite acceptable V. parahaemolyticus levels detected by routine testing of shellfish in these areas, as of July 31, 2006, eight shellfish harvest areas in Washington had been closed to harvesting because their oysters were associated with this Vibrio illness outbreak. Oysters from these areas have been recalled by Washington state shellfish-control authorities. Shellfish bed monitoring is an important element of food-safety control but is not sufficient to prevent illnesses caused by Vibrio organisms. Because vibrios multiply rapidly, even low levels of V. parahaemolyticus in harvested products can rapidly increase to infectious levels if not rapidly refrigerated after harvest and maintained at proper temperatures during transport, processing, and storage (i.e., <50ºF [<10ºC]). Medical providers should request stool specimens from patients with acute gastroenteritis and a history of recent shellfish consumption. The microbiology laboratory analyzing the sample should be notified that Vibrio illness, or vibriosis, is suspected so that appropriate methods (ideally, culture in the selective medium thiosulfate-citrate-bile salts-sucrose [TCBS] agar) can be used to isolate the organisms. Vibrio species grow readily in blood agar, but primary isolation of the organisms from stool samples is problematic because extensive screening is required to differentiate vibrios from other enteric organisms (5). Vibrio species infections should be reported to the appropriate health jurisdiction. Although infection with V. parahaemolyticus is not currently a nationally notifiable disease (as is cholera, the disease caused by cholerigenic strains of Vibrio cholerae),* CDC has conducted voluntary case surveillance for laboratory-confirmed noncholera Vibrio species infection since 1988. In June 2006, the Council of State and Territorial Epidemiologists recommended that all Vibrio species infections be classified as nationally notifiable diseases. The current outbreak underscores the benefits of coordinated national surveillance. Consumption of raw or undercooked shellfish is a recurrent source of human illness, including sporadic infections and widespread outbreaks. In recent years, the most commonly reported pathogens associated with these infections have been V. parahaemolyticus, Vibrio vulnificus, and norovirus, but outbreaks of hepatitis A and cholera also have been reported. To decrease the risk for V. parahaemolyticus infection, shellfish should be thoroughly cooked to kill illness-causing pathogens.† In two of the New York City clusters in this report, vibriosis was associated with cooked seafood (e.g., cooked lobster, scallops, crab, or shrimp) that was eaten in a restaurant, suggesting that the food might have been cross-contaminated by raw shellfish after cooking. Some commercially available oysters have been treated after harvest to reduce the levels of Vibrio bacteria. Improved surveillance for V. parahaemolyticus, in addition to increased use of postharvest treatment to decrease Vibrio species levels, and careful postharvest temperature control of shellfish during transport, processing, and storage are critical to limiting V. parahaemolyticus infections. Reported by: S Balter, H Hanson, L Kornstein, L Lee, V Reddy, S Sahl, F Stavinsky, New York City Dept of Health and Mental Hygiene; M Fage, G Johnson, New York State Dept of Health. J Bancroft, W Keene, Oregon Dept of Human Svcs. J Koepsell, M Williams, Public Health Seattle and King County; K MacDonald, N Napolilli, J Hofmann, Washington State Dept of Health. C Bopp, M Lynch, K Moore, J Painter, N Puhr, P Yu, Div of Foodborne, Bacterial, and Mycotic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases (proposed), CDC. * The Nationally Notifiable Diseases Surveillance System is a public health surveillance system that collects data on cases of certain diseases. The decision to make a disease nationally notifiable is based on its public health importance (e.g., number of cases or severity of the disease) and its preventability. The current list of nationally notifiable diseases is available at http://www.cdc.gov/epo/dphsi/phs/infdis.htm. † Cooking guidelines vary for each type of shellfish and are available from FDA at http://www.cfsan.fda.gov/~lrd/seafsafe.html or by telephone (888-723-3366). References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/10/2006 |
|||||||||
|