|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
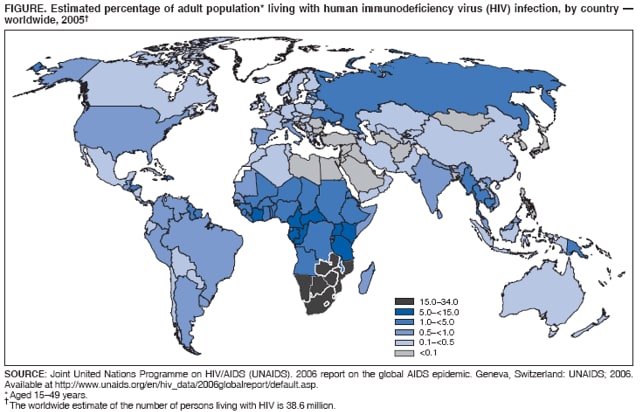
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. The Global HIV/AIDS Pandemic, 2006Please note: An erratum has been published for this article. To view the erratum, please click here. Since the first cases of acquired immunodeficiency syndrome (AIDS) were reported in 1981, infection with human immunodeficiency virus (HIV) has grown to pandemic proportions, resulting in an estimated 65 million infections and 25 million deaths (1,2). During 2005 alone, an estimated 2.8 million persons died from AIDS, 4.1 million were newly infected with HIV, and 38.6 million were living with HIV (2). HIV continues to disproportionately affect certain geographic regions (e.g., sub-Saharan Africa and the Caribbean) (Figure) and subpopulations (e.g., women in sub-Saharan Africa, men who have sex with men [MSM], injection-drug users [IDUs], and sex workers). Effective prevention and treatment of HIV infection with antiretroviral therapy (ART) are now available, even in countries with limited resources (2). Nonetheless, comprehensive programs are needed to reach all persons who require treatment and to prevent transmission of new infections. This report, published on the eve of the sixteenth International AIDS Conference (August 13--18, 2006, in Toronto, Canada), summarizes selected regional trends in the HIV/AIDS pandemic, based largely on data from the 2006 Report on the Global AIDS Epidemic by the Joint United Nations Programme on HIV/AIDS (UNAIDS) (2). Related reports in this issue of MMWR describe the prevalence of HIV infection among MSM in Thailand, HIV-related practices at chest clinics in Guyana, and HIV-related risk behaviors among high school students in the United States. Sub-Saharan Africa. Approximately 10% of the world population lives in sub-Saharan Africa, but the region is home to approximately 64% of the world population living with HIV (2). Transmission is primarily through heterosexual contact, and more women are HIV infected than men. Southern Africa is the epicenter of the AIDS epidemic; all countries in the region except Angola have an estimated adult (i.e., aged 15--49 years) HIV prevalence exceeding 10% (2). In Botswana, Lesotho, Swaziland, and Zimbabwe, the estimated adult HIV prevalence exceeds 20% (2). South Africa, with an HIV prevalence of 18.8% and 5.5 million persons living with HIV, has, along with India, the largest number of persons living with HIV in the world (2). Recently, declines in adult HIV prevalence have been observed in Kenya, Uganda, Zimbabwe, and urban areas of Burkina Faso. Although in these countries, HIV-related sexual risk behaviors and HIV incidence have decreased, AIDS death rates continue to rise. In sub-Saharan Africa, 17% of the estimated number of persons in need of ART received it in 2005 (3). Asia. Adult HIV prevalence is lower in Asian countries than in countries in sub-Saharan Africa, and the epidemic in most Asian countries is attributable primarily to various high-risk behaviors (e.g., unprotected sexual intercourse with sex workers, IDUs, or MSM and injection-drug use). Of the 8.3 million HIV-infected persons in Asia, 5.7 million live in India, where the prevalence varies by state. Approximately 80% of HIV infections in India are acquired heterosexually. Recent data from four Indian states indicated a decline in HIV prevalence among pregnant women aged 15--24 years, from 1.7% in 2000 to 1.1% in 2004 (4). In China, where 650,000 IDUs account for approximately half of persons living with HIV infection; in contrast, the epidemics in Thailand and Cambodia have been driven largely by commercial sex. In Thailand, HIV prevalence in pregnant women declined from 2.4% in 1995 to 1.2% in 2003. However, HIV prevalence among MSM in Bangkok increased from 17% in 2003 to 28% in 2005 (5). Only 16% of persons in need of ART in Asia received it in 2005 (3). Americas. HIV infections are reported mostly among MSM, IDUs, and sex workers in the Americas. Brazil, the second most populous country in the Americas (after the United States), has an adult HIV prevalence of 0.5% and has approximately 30% of the population living with HIV in South and Central America and the Caribbean. High-risk behavior among Brazilians aged 15--24 years remains high; one in three report initiating sexual activity before age 15 years, and one in five report having had more than 10 sex partners. Brazil provides free ART to all in need of treatment, and approximately 83% of HIV-infected persons receive therapy. After sub-Saharan Africa, the Caribbean is the second most HIV-affected region of the world. Like sub-Saharan Africa, HIV transmission in the Caribbean is largely heterosexual. HIV prevalence has declined in urban areas of Haiti but has remained constant in other areas of the Caribbean. Overall in South and Central America and the Caribbean, approximately 68% of persons in need of ART received it in 2005 (3). In the United States, recent evidence suggests a resurgence of HIV transmission among MSM; during 2001--2004, an estimated 44% of new HIV infections were in MSM, and 17% were in IDUs (6). In addition, blacks and Hispanics together account for 69% of all reported HIV/AIDS cases. In the United States, 55% of persons in need of ART received it in 2005. Reported by: World Health Organization, Geneva, Switzerland. Interagency Surveillance and Survey Working Group, Office of the US Global AIDS Coordinator, US Dept of State. Div of Global AIDS, National Center for HIV, Viral Hepatitis, STDs, and Tuberculosis Prevention (proposed), CDC. Editorial Note:This report summarizes certain regional trends in the HIV/AIDS pandemic, which has reversed the course of human development (7) and eroded improvements in life expectancy in countries with the highest prevalence of infection (2). The greatest HIV burden is in sub-Saharan Africa, home to 15 countries with the highest prevalence of HIV infection in the world. In most other regions, HIV infections have been concentrated in various high-risk populations. To be effective, prevention measures must be tailored to the local epidemiology of HIV infection, based on the behaviors and exposures associated with new transmission. From 2003 to 2005, estimates of adult HIV prevalence were lowered in many countries. Some of these reductions might be attributable to the addition of new surveillance sites and population-based surveys that provide better estimates in rural populations, which usually have lower HIV prevalence. However, some countries (including Kenya, Uganda, Zimbabwe, and urban parts of Burkina Faso and Haiti) have reported evidence of actual declines in HIV prevalence. Changes in sexual behavior (e.g., delayed initiation of sexual intercourse, decrease in number of sex partners, or increase in condom use) appear at least partly responsible for these declines, although increasing mortality might have been a contributing factor (8). During 2003--2005, substantial gains were made in the number of persons receiving ART in resource-limited countries (3). The "3 by 5" initiative, a strategy of the World Health Organization and UNAIDS, sought to provide treatment to 3 million persons (50% of those in need of treatment worldwide) in low- and middle-income countries by 2005. By December 2005, 18 countries had met their "3 by 5" target, and the number of persons receiving ART had increased from 400,000 in December 2003 to 1.3 million (3). Overall, this 225% increase can be attributed to commitments by the President's Emergency Plan for AIDS Relief (PEPFAR); the Global Fund To Fight AIDS, Tuberculosis, and Malaria; and the World Bank. By the end of March 2006, PEPFAR supported ART for 561,000 persons in 15 countries (9). Despite the gains in ART, only 20% of persons in need of treatment in low- and middle-income countries were receiving it in December 2005 (3). Despite a 5-year scale-up of interventions to prevent mother-to-child transmission (PMTCT) of HIV, approximately one in 10 pregnant women were offered PMTCT services, and fewer than one in 10 HIV-positive pregnant women received ART prophylaxis for PMTCT (2). Expansion of HIV testing, including the routine offer of testing and counseling in clinical settings, will be needed to identify more persons in need of ART and PMTCT services; improvements in infrastructure and human resources will be needed to deliver quality services to the increasing number of persons requiring treatment. As more HIV-infected persons receive ART, the number of persons living with HIV infection will increase, requiring that prevention programs scale up to prevent HIV transmission from those living with HIV infection and for those at risk for infection. Prevention measures directed toward populations most likely to be exposed to HIV in low-level and concentrated epidemics* and toward young persons and those with HIV infection in generalized epidemics must be scaled up in parallel with care and treatment programs. To maximize the effectiveness of HIV/AIDS programs, the quality and coverage of services should be evaluated, and the success of interventions should be assessed by analyzing trends in morbidity, mortality, and behaviors of populations infected with HIV or at risk for HIV infection. Using these data to modify and improve HIV/AIDS programs, an approach integrating prevention and treatment is being developed that could reduce treatment need by as much as 50% by 2020 (10). * WHO and UNAIDs define these three types of epidemics as follows: low level: HIV prevalence has not consistently exceeded 5% in any defined subpopulation; concentrated: HIV prevalence is consistently >5% in at least one defined subpopulation and is <1% in pregnant women in urban areas, and generalized: HIV prevalence is consistently >1% in pregnant women. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/10/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|