|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
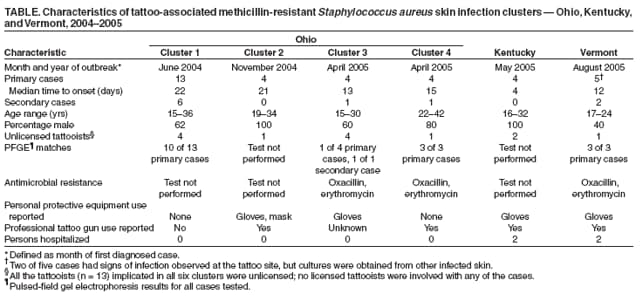
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Methicillin-Resistant Staphylococcus aureus Skin Infections Among Tattoo Recipients --- Ohio, Kentucky, and Vermont, 2004--2005Community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) infections have emerged as a major cause of skin disease in the United States (1). Outbreaks of CA-MRSA have occurred among athletes, inmates at correctional facilities, and military recruits (2--4). This report summarizes investigations of six unlinked clusters of skin and soft tissue infections caused by CA-MRSA among 44 recipients of tattoos from 13 unlicensed tattooists in three states (Ohio, Kentucky, and Vermont); use of nonsterile equipment and suboptimal infection-control practices were identified as potential causes of the infections. Clinicians should consider CA-MRSA in their differential diagnosis for staphylococcus diseases, including skin infections. Clinicians can contact their local health departments to determine the prevalence of CA-MRSA in their community and whether the disease is reportable. MRSA infections should be added to education and prevention campaigns highlighting the risks of unlicensed tattooing. CA-MRSA outbreaks among tattoo recipients were identified by hospital infection-control practitioners and reported to local health departments in six separate communities in Ohio, Kentucky, and Vermont during June 2004--August 2005 (Table). CA-MRSA is reportable in Ohio, Kentucky, and Vermont during outbreaks or when clusters have been identified. CDC was notified independently of the clusters in Ohio (four clusters) and Kentucky (one) by the state health departments; the Vermont Department of Health notified public authorities nationally of one tattoo-associated CA-MRSA cluster in August 2005 by using the Epidemic Information Exchange (Epi-X). After this notification, CDC contacted the Vermont Department of Health to share information on the clusters. Separate investigations of each cluster were conducted by local and state health departments, assisted by CDC, to identify the sources of exposure. A primary case of tattoo-associated CA-MRSA skin infection was defined as a skin infection consistent with staphylococcal infection (e.g., boil, folliculitis, erythema, or abscess) that occurred near or at the site of a recent tattoo in a person from whom a culture from that site yielded MRSA. A secondary case was defined as a skin infection consistent with staphylococcal disease that occurred in a person who had not received a recent tattoo, had provided a specimen that yielded MRSA, and had been in close contact with an MRSA patient who had received a tattoo. A total of 34 primary cases and 10 secondary cases were identified in the three states. Patients ranged in age from 15 to 42 years. The majority were male (73%) and white (63%); 35% were black. Except for one Ohio patient with hepatitis C, no underlying diseases or risk factors were identified. Among all 34 primary cases, the time from tattoo to symptom onset was 4--22 days; no incubation period was recorded for the secondary cases described in this report. Most infections were mild to moderate, ranging from cellulitis and small pustules (Figure) to larger abscesses that required surgical incision and drainage (n = 20). Most infections improved with surgical drainage (n = 16) and/or oral antimicrobials (n = 24), including trimethoprim-sulfamethoxazole, levofloxacin, and clindamycin. Four patients had bacteremia and required hospitalization for intravenous vancomycin. During interviews regarding the circumstances of their tattoos, 34 patients with primary MRSA identified a total of 13 unlicensed tattooists. Investigations were performed by local health departments in coordination with law enforcement officials; seven tattooists who could be located were interviewed. Although gloves were reportedly worn by all tattooists in four of the six clusters (defined by spatial and temporal relationships), adherence to other infection-control measures (e.g., changing gloves between clients and performing appropriate hand hygiene, skin antisepsis, and disinfection of equipment and surfaces) was not practiced. Investigators determined that three of the tattooists in Ohio had recently been incarcerated in correctional facilities, a potential site for exposure to MRSA infection (4). However, none of the tattooists from Kentucky or Vermont reported previous incarceration. None of the 34 persons with primary cases were incarcerated when they received their tattoos. Five patients reported seeing lesions on the hands of tattooists that were consistent in description with MRSA skin infection, and one tattooist reported a pustule on his finger; however, no specimens from tattooists were cultured. All 13 primary patients in the first of the four Ohio clusters reported receiving their tattoos in public places (e.g., parks or private residences) from tattooists who used homemade tattooing equipment consisting of guitar-string tattoo needles and computer ink-jet printer cartridges for dye. The persons with secondary cases were exposed to persons with primary cases by direct contact because they were living in the same house or had close personal contact. Isolates from four of the six clusters also were characterized by pulsed-field gel electrophoresis (PFGE). Analysis of PFGE results revealed that isolates were indistinguishable within each cluster and all were USA300, a common CA-MRSA type (Table). Antimicrobial susceptibilities were characterized for infections in two of the Ohio clusters and the Vermont cluster. S. aureus isolates in all three clusters were resistant to oxacillin and erythromycin. Interventions initiated by local health departments included educational forums targeting local infection-control professionals and medical providers. Students also were targeted in one Ohio community because many of the cases occurred in persons who attended one local high school and the educational forums provided them with information regarding the dangers of illegal tattoos. In addition, public service announcements were issued on the radio and in local newspapers, discussing the risks of acquiring tattoos from unlicensed tattooists and the possibility of skin infections with CA-MRSA. Reported by: T Long, MD, D Coleman, MS, P Dietsch, P McGrath, D Brady, Columbus Health Dept, Columbus; D Thomas, MPH, Toledo-Lucas County Health Dept, Toledo; T Corzatt, Highland County Health Dept, Hillsboro; M Ruta, Columbiana County Health Dept, Lisbon; R Duffy, DDS, E Koch, MD, Ohio Dept of Health. S Trent, Gateway District Health Dept, Owingsville, Kentucky. N Thayer, J Heath, MEd, S Schoenfeld, MSPH, C Lohff, MD, Vermont Dept of Health. J Hageman, MHS, D Jernigan, MD, Div of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases (proposed); M LeMaile-Williams, MD, EIS Officer, CDC. Editorial Note:CA-MRSA skin infections are usually transmitted from person to person by direct contact with a draining lesion or by contact with an asymptomatic carrier of S. aureus. Transmission also can occur indirectly through contact with contaminated items or environmental surfaces (3,5). In 2001, CDC initiated population-based surveillance for CA-MRSA at three Emerging Infection Program (EIP) sites using the Active Bacterial Core surveillance (ABCs) program (1). Currently, nine EIP sites participate in ABCs invasive MRSA surveillance, which represents a population of 16.3 million persons.* The annual incidence for all MRSA infections varied from 18.0 to 25.7 cases per 100,000 population. The majority of these were skin and soft tissue infections, accounting for 75% of cases (1). Limited data are available on the morbidity and mortality of CA-MRSA. Most infections are mild skin and soft tissue infections, but more severe invasive disease such as pneumonia and necrotizing fasciitis has been reported (6,7). The cases in this report involved persons who received services from unlicensed tattooists who reportedly did not follow proper infection-control precautions recommended by tattoo industry groups and local and state regulators. These recommendations include following infection-control standard precautions† and using sterilized or single-use equipment, including needles, tattoo guns, and ink supplies. Persons considering getting a tattoo should be aware of the potential for CA-MRSA infection associated with unlicensed tattooists. Laws and regulating authorities for tattooing vary by state. In Ohio, tattooing is regulated by local health departments,§ in Vermont by the Office of the Secretary of State,¶ and in Kentucky by the State Cabinet for Health Services.** Statutes or regulations have been in place in these three states since the mid-1990s. For example, under Ohio law, the operator of a tattoo establishment must ensure that tattooists follow standard infection-control procedures, are trained adequately, and have completed required first aid and bloodborne pathogen courses. Certain states have reported an increase in CA-MRSA infections in their prisons (4). In this report, three of the tattooists associated with outbreaks in Ohio had been incarcerated recently. However, the prevalence of unlicensed tattooists in Ohio and other states is unknown; similarly, any association between CA-MRSA infection and tattooists who have been incarcerated is unknown. In response to the outbreaks described in this report, local health departments rapidly targeted members of the affected population and health-care providers with CA-MRSA prevention messages and provided recommendations for early treatment of infections. Since implementation of the campaigns, no new CA-MRSA clusters have been reported in the affected areas. Persons considering a tattoo should be aware of the potential for CA-MRSA infection and should only use the services of a licensed tattooist who follows proper infection-control procedures. References
* Available at http://www.cdc.gov/ncidod/dhqp/ar_mrsa_CDCactions.html. † Available at http://www.cdc.gov/ncidod/dhqp/gl_isolation_standard.html. § Ohio Revised Code, Sections 3730.01--3730.11; 1997; Ohio Administrative Code, Chapter 3701-9; 1998. Available at http://onlinedocs.andersonpublishing.com/oh/lpExt.dll?f=templates&fn=titlepage.htm. ¶ The Vermont Statutes, Title 26, Chapter 79. Tattooists and Body Piercers; 2004. Available at http://www.leg.state.vt.us/statutes/fullsection.cfm?Title=26&Chapter=079&Section=04103. ** Kentucky Tattoo Regulation; 2004; Kentucky Tattoo and Body Piercing Law; 2005. Available at http://www.lrc.state.ky.us/krs/211-00/760.pdf.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 6/22/2006 |
|||||||||
|