|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
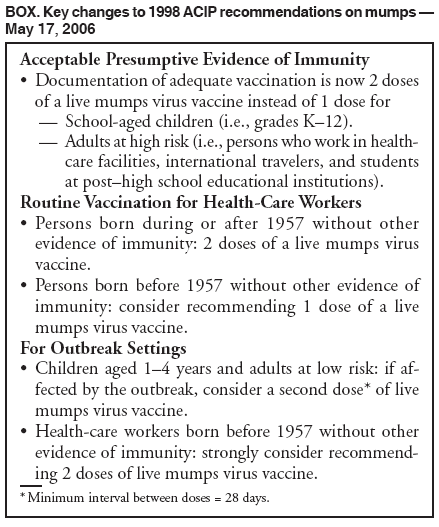
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Notice to Readers: Updated Recommendations of the Advisory Committee on Immunization Practices (ACIP) for the Control and Elimination of MumpsOn June 1, this notice was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr). On May 17, 2006, the Advisory Committee on Immunization Practices (ACIP) updated criteria for mumps immunity and mumps vaccination recommendations. According to the 1998 ACIP recommendations for measles, mumps, and rubella (MMR) vaccine, for routine vaccination, a first dose of MMR vaccine is recommended at ages 12--15 months and a second dose at ages 4--6 years. Two doses of MMR vaccine also are recommended for students attending colleges and other post--high school institutions (1). However, documentation of mumps immunity through vaccination has consisted of only 1 dose of mumps-containing vaccine for all designated groups, including health-care workers. Live mumps virus vaccines (i.e., mumps and MMR vaccines) produced in the United States are derived from the Jeryl Lynn mumps vaccine strain. Postlicensure studies in the United States demonstrated that 1 dose of mumps vaccine was 78%--91% effective in preventing clinical mumps with parotitis (2). However, in the late 1980s and early 1990s, mumps outbreaks were observed in schools with extremely high (>95%) vaccination coverage (3,4), suggesting that 1 dose of mumps vaccine or MMR vaccine was not sufficient to prevent mumps outbreaks in school settings. In response to the resurgence of measles that began in 1989 and continued through 1991 (1), a second dose of MMR vaccine for school-aged (i.e., grades K--12) and college students was recommended in 1989. Since implementation of the 2-dose MMR vaccination requirement, the incidence of mumps disease has decreased, and studies of vaccine effectiveness during outbreaks suggest substantially higher levels of protection with a second dose of MMR. For example, during a mumps outbreak at a Kansas high school during the 1988--89 school year, students who had received only 1 dose of MMR had five times the risk of contracting mumps compared with students who had received 2 doses (3). A study from the United Kingdom, which uses MMR vaccines that contain either the Jeryl Lynn mumps vaccine strain or the RIT 4385 strain (derived from the Jeryl Lynn strain) (2), indicated a vaccine effectiveness of 88% for 2 doses of MMR vaccine compared with 64% for a single dose (5). In addition, elimination of mumps was declared in Finland through high and sustained coverage with 2 doses of MMR vaccine (6). Infection-control failures resulting in nosocomial transmission have occurred during mumps outbreaks involving hospitals and long-term--care facilities that housed adolescent and young adult patients (7). Exposures to mumps in health-care settings also can result in added economic costs associated with furlough or reassignment of staff members from patient-care duties or closure of wards. During January 1--May 2, 2006, the current outbreak in the United States has resulted in reports of 2,597 cases of mumps in 11 states (8). The outbreak has underscored certain limitations in the 1998 recommendations relating to prevention of mumps transmission in health-care and other settings with high risk for mumps transmission. After reviewing data from the current outbreak and previous evidence on mumps vaccine effectiveness and transmission, ACIP issued updated recommendations for mumps vaccination (Box). Acceptable Presumptive Evidence of Immunity to MumpsAcceptable presumptive evidence of immunity to mumps includes one of the following: 1) documentation of adequate vaccination, 2) laboratory evidence of immunity, 3) birth before 1957, or 4) documentation of physician-diagnosed mumps. Evidence of immunity through documentation of adequate vaccination is now defined as 1 dose of a live mumps virus vaccine for preschool-aged children and adults not at high risk and 2 doses for school-aged children (i.e., grades K--12) and for adults at high risk (i.e., health-care workers,* international travelers, and students at post--high school educational institutions).† Routine Vaccination for Health-Care WorkersAll persons who work in health-care facilities should be immune to mumps. Adequate mumps vaccination for health-care workers born during or after 1957 consists of 2 doses of a live mumps virus vaccine. Health-care workers with no history of mumps vaccination and no other evidence of immunity should receive 2 doses (at a minimum interval of 28 days between doses). Health-care workers who have received only 1 dose previously should receive a second dose. Because birth before 1957 is only presumptive evidence of immunity, health-care facilities should consider recommending 1 dose of a live mumps virus vaccine for unvaccinated workers born before 1957 who do not have a history of physician-diagnosed mumps or laboratory evidence of mumps immunity. Mumps Outbreak ControlDepending on the epidemiology of the outbreak (e.g., the age groups and/or institutions involved), a second dose of mumps vaccine should be considered for children aged 1--4 years and adults who have received 1 dose. In health-care settings, an effective routine MMR vaccination program for health-care workers is the best approach to prevent nosocomial transmission. During an outbreak, health-care facilities should strongly consider recommending 2 doses of a live mumps virus vaccine to unvaccinated workers born before 1957 who do not have evidence of mumps immunity. These new recommendations for health-care workers are intended to offer increased protection during a recognized outbreak of mumps. However, reviewing health-care worker immune status for mumps and providing vaccine during an outbreak might be impractical or inefficient. Therefore, facilities might consider reviewing the immune status of health-care workers routinely and providing appropriate vaccinations, including a second dose of mumps vaccine, in conjunction with routine annual disease-prevention measures such as influenza vaccination or tuberculin testing. References
* Health-care workers include persons who provide health care to patients or work in institutions that provide patient care (e.g., physicians, nurses, emergency medical personnel, dental professionals and students, medical and nursing students, laboratory technicians, hospital volunteers, or administrative and support staff in health-care institutions). † The first dose of mumps-containing vaccine should be administered on or after the first birthday; the second dose should be administered no earlier than 1 month (i.e., at a minimum of 28 days) after the first dose. MMR vaccine generally should be used whenever any of its component vaccines are indicated. For children aged 12 months--12 years, combined measles, mumps, rubella, and varicella (MMRV) vaccine can be considered if varicella vaccination is also indicated.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 6/7/2006 |
|||||||||
|