|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
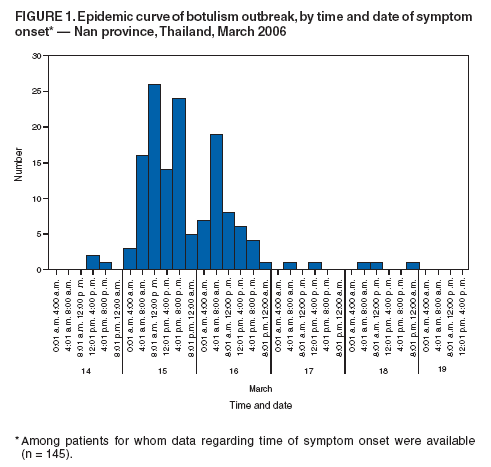
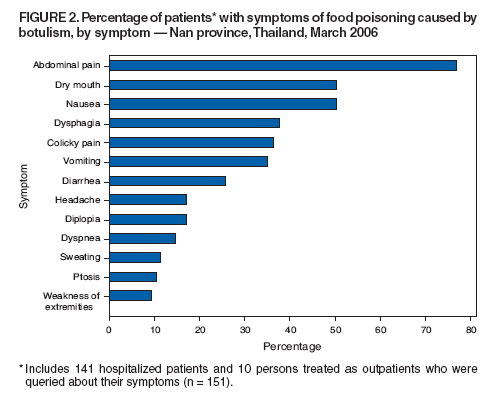
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Botulism from Home-Canned Bamboo Shoots --- Nan Province, Thailand, March 2006Please note: An erratum has been published for this article. To view the erratum, please click here. On March 15, 2006, multiple persons with symptoms of nausea, vomiting, abdominal pain, and dyspnea visited the emergency department at Baan Luang district hospital in Nan province, Thailand; one person required mechanical ventilation. A team from the Bureau of Epidemiology, Department of Disease Control, Thailand Ministry of Public Health (MOPH) initiated an investigation, in collaboration with the Surveillance and Rapid Response Team from Baan Luang district. This report summarizes the investigation conducted during March 15--26, which determined that the outbreak was caused by foodborne botulism from home-canned bamboo shoots and affected 163 rural villagers who shared a common meal. The last case was identified March 21; no further cases of foodborne botulism have been identified in the region. On March 14, an annual religious rite was observed in Nawaimai village, Pakaluang subdistrict, Baan Luang district, Nan province. Villagers from Pakaluang and neighboring subdistricts joined the event. That day, several persons who attended the festival visited local health-care providers with symptoms of gastroenteritis. Personnel from the MOPH Field Epidemiology Training Program (FETP) were notified of a possible foodborne outbreak on March 15. Illnesses progressed to include bulbar muscle paralysis, with respiratory depression requiring ventilatory support in three patients, at which time a botulism outbreak was suspected. A quick door-to-door survey conducted by village volunteers identified 354 villagers who had attended the event, of whom 200 (56%) ate food served at the event. A case was defined as one or more symptoms* of food poisoning in a person who attended the religious rite. Active case finding among health facilities and communities in the affected districts was initiated; all provinces were asked to report patients with similar symptoms. During March 15--26, a total of 163 persons (82% of the 200 persons who ate at the festival) had illness consistent with the case definition. The median age of ill persons was 45 years (range: 13--75 years); 113 (69%) were female. The first patient had illness onset at 2:00 p.m. on March 14, and 87 (53%) patients had illness onset on March 15 (Figure 1). The last patient had illness onset on March 18. Of the 163 persons with illness, 141 (86.5%) were admitted to area hospitals. All 141 hospitalized patients and 10 patients treated as outpatients were systematically queried about their symptoms (Figure 2). The majority of those patients experienced abdominal pain (116; 76.8%), dry mouth (76; 50.3%), and nausea (76; 50.3%); some had dysphagia (52; 37.7%), vomiting (53; 35.1%), diplopia (26; 17.2%), ptosis (16; 10.6%), and weakness of extremities (14; 9.3%). Forty-two (29.8%) of the hospitalized patients required mechanical ventilation. Local public health officials and FETP epidemiologists interviewed 145 of 200 persons who attended the festival by using a standard questionnaire to assess food consumed and possible illness. Food served at the religious rite included home-canned bamboo shoots eaten with chili and shrimp paste, wax gourds, chicken curry, sticky rice, water, and ice. Home-canned bamboo shoots were the only item eaten by 100% of affected persons, although bamboo shoots were routinely consumed with the chili and shrimp paste. The bamboo shoots had been produced locally by a women's group in the village. The shoots had been processed in 20-liter cans with approximately 13 kg of shoots per can. A total of 53 cans were produced during September 2005; 46 cans were sold during September 2005--February 2006, primarily in the district where they were made. No other recent reports of similar illness in the area occurred before this outbreak. The morning of the day of the festival, bamboo shoots from two cans had been combined, washed and sliced into pieces, and placed into plastic bags before being distributed at lunch. One food preparer reported that one of the two cans of bamboo shoots appeared turbid before mixing, but the bamboo shoots were not discarded. On the basis of clinical manifestations of the patients and results of the epidemiologic investigation, the most probable cause of illness was botulinum toxin from Clostridium botulinum. Samples of the leftover canned bamboo shoots were cultured by the MOPH Department of Medical Sciences on March 20 and grew C. botulinum on March 24. On April 10, multiplex polymerase chain reaction identified toxin type A. Thai and CDC scientists are collaborating to test patient specimens, including serum, vomitus, and gastric fluid. Because of the cluster of patients with symptoms consistent with botulism, the number of patients requiring mechanical ventilation, and the progression of disease in several villagers, MOPH requested assistance from international partners in obtaining botulism antitoxin; no local source of antitoxin was available. Twenty vials of heptavalent antitoxin (A--G) were provided by the United Kingdom Department of Health with assistance from the World Health Organization, 50 vials of bivalent antitoxin (A, B) were donated by CDC, and 23 vials of trivalent antitoxin (A, B, E) were donated by the National Institute of Infectious Diseases in Japan. Thailand purchased an additional 10 vials of bivalent antitoxin (A, B) from a Canadian company. Antitoxin was administered to patients with the most severe symptoms; 70 vials were administered on March 19 and 20, and the last of the 93 vials used was administered on March 23. Although published data suggest that antitoxin is most effective if administered within the first 24 hours of illness onset (1), botulism antitoxin was administered to patients later in the course of illness to halt the progression of paralysis and potentially shorten the duration of illness. A study to assess the short- and long-term outcomes of a subset of patients is under way. On March 21, a team of critical care specialists (pulmonologists, a neurologist, and a toxicologist) from Bangkok traveled to Nan province to assess the respiratory care capabilities in the province. Because patients with severe botulism might remain on a ventilator for a month or longer requiring round-the-clock care, 26 patients were transferred on March 22 by the Thai Air Force to neighboring provincial hospitals and to tertiary care hospitals in Bangkok for long-term respiratory care. As of April 10, a total of 25 patients remained hospitalized, and 9 (36%) were still on respirators; no patients had died. Reported by: Surveillance and Rapid Response Teams from Baan Luang district and Nan Provincial Health Office; Nan Provincial Hospital; Office of Disease Prevention and Control 10, Dept of Disease Control (DDC), Ministry of Public Health (MOPH), Chiang Mai; Field Epidemiology Training Program, Bur of Epidemiology, DDC, MOPH; Thailand MOPH--U.S. CDC Collaboration; World Health Organization representative to Thailand, Nonthaburi, Thailand. Div of Foodborne, Bacterial and Mycotic Diseases, National Center for Zoonotic, Vector-Borne and Enteric Diseases, CDC. Editorial Note:In 1998, a smaller outbreak of botulism associated with home-canned bamboo shoots was reported in the same Thai province (2). Recommendations for home-canned food production were disseminated widely to all provinces. However, this recurrence 8 years later indicates the importance of long-term follow up and continuous inspection and assurance of the quality of food canning. As a result of this investigation, MOPH recommended increasing control of home-canned food production in all provinces and strengthening surveillance for foodborne botulism. The provincial government prohibited sale of all leftover cans and advised the population to buy only Thai Food and Drug Administration--approved, commercially canned food products, to boil home-canned bamboo shoots for 10 minutes before eating, and to discard cans with defects (e.g., dents, swelling, discoloration, rust, or foul smell). Warnings about the outbreak were issued through local radio stations and the Internet, with educational messages about proper preparation of bamboo shoots for home canning. On March 20, health officials collected 21 leftover cans and approximately 550 plastic bags of bamboo shoots from three producers in Baan Luang district. In addition, provincial health officials are strengthening surveillance activities for botulism; a notice was sent to all hospitals and district health centers to urge clinicians and public health professionals to report any persons with signs or symptoms consistent with botulism. Local health authorities will continue to monitor persons who ate the shared meal until all signs of associated illness have resolved. The current outbreak tested the rapid response capabilities of several countries. Surveillance and Rapid Response Teams in Thailand, who are trained to detect and respond to public health emergencies, were rapidly deployed. A quick assessment identified a large foodborne outbreak, with no malicious intent suspected (3). In addition, the World Health Organization and CDC rapidly identified and procured sources of antitoxin. This outbreak response highlights the importance of communication and collaboration between local health authorities and international health agencies. References
* Abdominal pain, colicky pain, nausea, vomiting, diarrhea, headache, sweating, dry mouth, dysphagia, diplopia, ptosis, weakness of extremities, and dyspnea.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/13/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|