|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
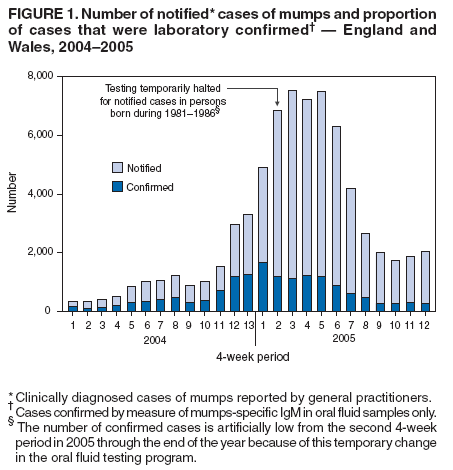
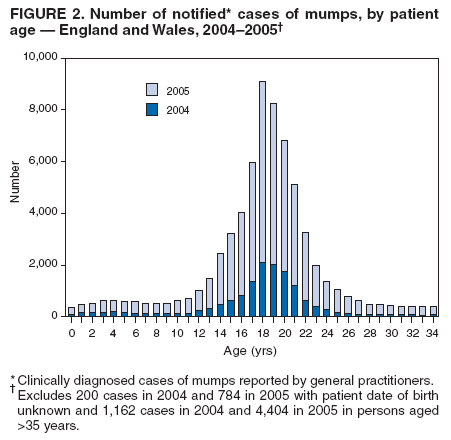
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Mumps Epidemic --- United Kingdom, 2004--2005During 2004--2005, the United Kingdom (UK) experienced a nationwide epidemic of mumps, which peaked during 2005 when 56,390* notified cases were reported in England and Wales. The majority of confirmed cases during 2004--2005 were in persons aged 15--24 years, most of whom had not been eligible for routine mumps vaccination. Mumps usually is a self-limited viral disease that appears as parotitis. However, mumps also can lead to serious complications such as encephalitis or pancreatitis. This report summarizes the epidemiology of the 2004--2005 mumps epidemic in England and Wales. Reporting was based on notified cases (i.e., clinically diagnosed cases of mumps reported by general practitioners). Since late 1994, laboratory confirmation of all notified cases of mumps has been recommended using a test to detect mumps-specific IgM antibodies in either serum or an oral fluid (1). The proportion of such cases began to increase in 1999 and increased further in each subsequent year, indicating an increase in the incidence of true infection. The number of notified cases began increasing in 2003 and continued to increase during 2004--2005, accompanied by further increases in the proportion of confirmed cases (Figure 1). During 2004, a total of 16,367 cases were notified; 10,641 (65.0%) of these were tested for oral fluid IgM, and 6,047 of those cases (56.8%) were determined to be IgM positive. When combined with those cases confirmed by serum IgM testing, a total of 8,128 (49.7%) cases were laboratory confirmed during 2004, compared with 3,907 (29.9%) of 13,087 notified cases during 1999--2003. In February 2005, because of high rates of laboratory confirmation of cases among persons born during 1981--1986, the UK Health Protection Agency recommended a temporary halt to testing persons with notified cases of mumps born during those years (2), although persons in other age groups with lower rates of confirmation continued to be tested. Testing for all age groups resumed in January 2006 after a sustained decline in the number of notified cases in the last quarter of 2005. During 2004, approximately 79.1% of confirmed cases were in persons aged 15--24 years. Among all mumps patients during 2004, approximately 3.3% were reported as having received 2 doses of measles, mumps, and rubella (MMR) vaccine, and another 30.1% had received 1 dose of MMR. The number of notified cases of mumps continued to increase through the first 6 months of 2005, with 20,653 cases occurring during the first quarter and 21,981 cases during the second quarter. During the third quarter of 2005, the number of notified cases decreased by 64.0% to 7,907; during the fourth quarter, a further decrease to 5,882 notified cases was observed (Figure 1). During the first month of 2006, notified cases of mumps averaged approximately 500 per week. During 2005, the majority of notified mumps cases were in persons aged 19--23 years and attending colleges or universities (Figure 2); the third-quarter decrease in the number of notified cases coincided with summer vacations. Local health services have been encouraged by the UK Health Protection Agency to ensure that all students have received 2 doses of MMR before leaving school. In addition, many universities have advised enrolling first-year students to receive MMR vaccination before arriving at college. Reported by: E Savage, PhD, JM White, FFPH, DEW Brown, FRCPath, ME Ramsay, FFPH, Immunisation Dept, Health Protection Agency Centre for Infections, London, England. Editorial Note:In October 1988, mumps vaccination was added to the UK vaccination schedule as part of the new combined MMR vaccine. MMR replaced single measles vaccine offered at age 12--15 months; since 1996, a second dose of MMR has been offered at age 3.5--5 years. Vaccination coverage in the UK peaked during 1995, when 92% of children aged 2 years were reported as having received at least 1 dose of MMR. As of the second quarter of 2005, vaccination coverage with at least 1 dose by age 2 years had declined to 82%, with 75% of children having received 2 doses by age 5 years. During November 1994, approximately 8 million school children aged 5--16 years (i.e., born during September 1978--August 1989) were offered combined measles-rubella vaccine to prevent a predicted epidemic of measles. At that time, a global shortage prevented offering MMR to this group. Therefore, a proportion of the 8 million children remained susceptible to mumps. Modelling based on serologic surveillance data for 1993 estimated that 19% of children aged 11--15 years in 1997 (i.e., aged 19--23 years in 2005) would be susceptible to mumps (4). The 2004--2005 mumps epidemic in the UK did not result from the decrease in MMR vaccination coverage in recent years, but rather from gaps in eligibility of certain cohorts, which has been evident during the epidemic by the age breakdown among patients with confirmed cases; mumps occurred predominantly in older teens and young adults, with the highest attack rate occurring in those born during 1983--1986 (3). Persons born before September 1987 generally were not eligible for any routine mumps vaccination, although some might have received 1 dose of MMR upon school entry as part of a catch-up campaign after October 1988 that targeted children who missed their measles vaccination. Persons born before 1982 are more likely to have been exposed to mumps infection when it was still a common childhood disease. Only 2.4% of confirmed cases in 2004 occurred in persons who would have been eligible for 2 doses of MMR routinely. The UK epidemic illustrates the susceptibility of certain cohorts who have not been vaccinated and have not developed immunity through exposure to mumps because of a decrease in mumps circulation after implementation of a childhood immunization program. The epidemic also underscores the importance of ensuring high levels of mumps immunity among adolescents and young adults when vaccination with mumps-containing vaccine is introduced into the routine immunization schedule for children. References
* Provisional total.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/23/2006 |
|||||||||
|