|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
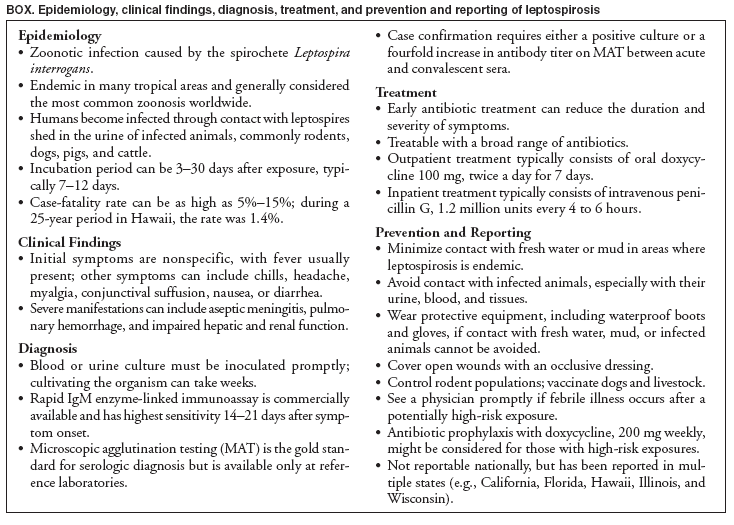
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Brief Report: Leptospirosis After Flooding of a University Campus --- Hawaii, 2004On November 19, 2004, the Hawaii Department of Health (HDOH) received a report that a University of Hawaii professor aged 56 years had been hospitalized with suspected leptospirosis after cleaning his flooded laboratory. On October 31, heavy rains had caused an adjacent stream to overflow its banks and flood the campus. Persons exposed to fresh water or mud contaminated by the urine of animals infected with the spirochete Leptospira interrogans can have systemic illness if the leptospires enter the body through broken skin or mucous membranes. This report describes the subsequent investigation by HDOH, assisted by CDC, which highlights the importance of maintaining clinical suspicion for leptospirosis after flooding in areas where the illness is endemic, even in well-developed urban settings. During October 31--November 2, the professor waded in his flooded laboratory in sandals, resulting in blisters. On November 10, he became ill with fever, chills, and vomiting. By November 14, the fever had subsided, but the man had other symptoms, including tremor, poor balance, and visual flashes of light. On November 17, his symptoms persisted; he went to a hospital emergency department and was hospitalized. Qualitative leptospiral IgM enzyme-linked immunoassay (EIA) of serum drawn on admission was negative. The physician continued to suspect leptospirosis, and the patient improved with a course of oral doxycycline. A second serum drawn November 24 tested positive for leptospirosis by IgM EIA. The patient's microscopic agglutination test (MAT) result was negative for the acute-phase specimen from November 17, but the convalescent-phase specimen drawn 7 days later revealed elevated titers to Leptospira antigens. Other persons participating in cleanup activities on the campus (e.g., university faculty, students, staff, employees of a commercial contractor, and members of the Civil Defense and National Guard) might have been exposed to leptospires. In collaboration with the university, HDOH established surveillance for febrile illness among members of the university community using a voluntary, Internet-based questionnaire, announced through the university e-mail system. Respondents were asked whether they had had contact with flood water and had become ill with fever after the flood. HDOH also conducted active case finding by contacting the Civil Defense, National Guard, and the contractor. Free testing for leptospirosis was offered through HDOH. A total of 271 persons responded to the Internet questionnaire, of whom 90 (33.2%) reported having a febrile illness within 30 days of having contact with flood water. Of the 90 persons reporting febrile illness, 34 (37.8%) reported seeing a physician; 46 (51.1%) were screened for leptospirosis using IgM EIA. Only one additional case of acute leptospirosis infection was identified. A male graduate student aged 27 years worked in the same laboratory as the professor and tested positive for leptospirosis by IgM EIA and MAT. He became ill on November 10 with fever, chills, vomiting, diarrhea, and headache. He recovered without treatment in 1 week but visited a physician for testing on November 19 after learning that his professor was ill with suspected leptospirosis. Leptospirosis is considered the most common zoonosis worldwide and is endemic in tropical environments such as Hawaii, where the mean annual incidence is 1.29 per 100,000 population (1). However, infection also can occur in milder climates, either as a result of local exposure or in travelers returning from the tropics. Natural disasters such as floods and hurricanes increase the risk for human exposure to leptospires through contact with contaminated water or mud.* Initial symptoms of leptospirosis resemble those of any influenza-like illness, with fever usually the only common symptom; therefore, a thorough exposure history is essential to diagnosis (Box). Although many infected persons recover spontaneously, 5%--10% of cases can progress to a more serious and potentially fatal second stage of illness that affects organ systems. Results from serologic testing for leptospiral antibodies or culture are not available rapidly enough to guide clinical decisions. Prompt, appropriate, empirical antibiotic therapy can prevent more severe disease (2). The optimal performance of IgM EIA is 14--21 days after symptom onset (3). However, the definitive serologic diagnostic assay for leptospirosis is the MAT, which requires technical expertise and maintenance of multiple live leptospiral serovars (2). This assay is available only at selected laboratories (including at CDC) in the network of World Health Organization Collaborating Centers for Leptospirosis. Persons participating in flood cleanup in areas where Leptospirae might be present should adopt appropriate protective measures, such as wearing waterproof boots (Box). Workers with broken skin should avoid contact with fresh water or mud; at minimum, open wounds should be protected with an occlusive dressing. Medical attention should be sought promptly by any person who has onset of febrile illness within 1 month of participating in the cleanup of a flood-affected area. Reported by: SY Park, MD, PV Effler, MD, M Nakata, D Sasaki, DVM, Hawaii Dept of Health; AR Katz, MD, Univ of Hawaii. TA Clark, MD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; K Gaynor, MD, EIS Officer, CDC. References
* Additional information is available at http://www.bt.cdc.gov/disasters/hurricanes/infectiousdisease.asp.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/8/2006 |
|||||||||
|