|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
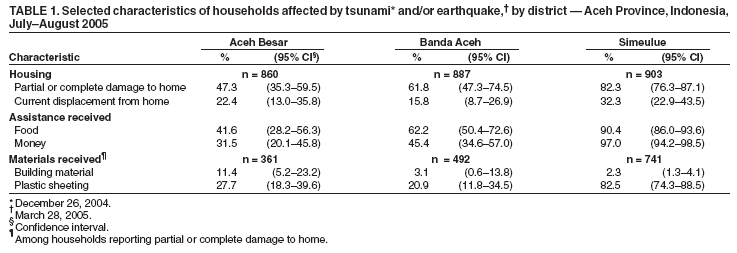
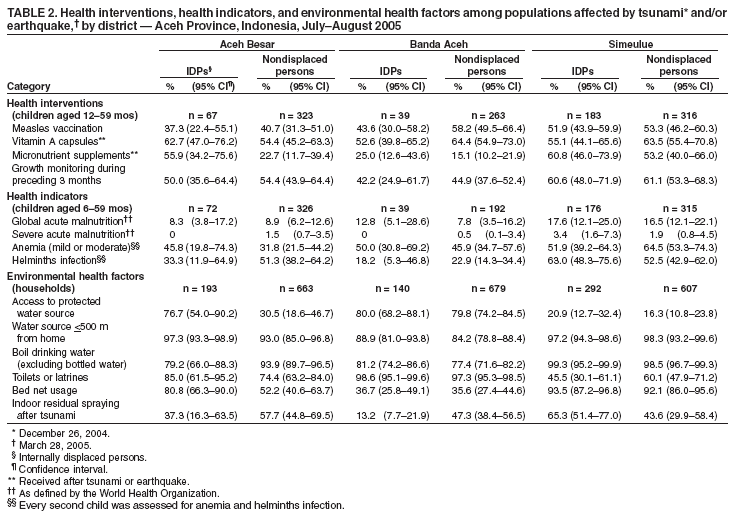
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Assessment of Health-Related Needs After Tsunami and Earthquake --- Three Districts, Aceh Province, Indonesia, July--August 2005On December 26, 2004, an earthquake measuring 9.2 on the Richter scale off the northwest coast of the island of Sumatra, Indonesia, produced a tsunami that caused the deaths of an estimated 230,000 persons in India, Indonesia, the Maldives, Somalia, Sri Lanka, and Thailand (1). The majority of casualties were in Aceh Province (population 4.5 million) in northern Sumatra, Indonesia, where an estimated 130,000 persons died. In addition, 500,000 persons were displaced from their homes, and 37,000 remain unaccounted for in the province. In the Aceh Province districts of Banda Aceh and Aceh Besar, an estimated 90,000 persons died (2); approximately 75% of health workers in Banda Aceh either died or were displaced from their homes (3). On March 28, 2005, a second major earthquake, measuring 8.7 on the Richter scale, caused large-scale damage to the islands of Simeulue and Nias off the western Sumatra coast; approximately 300 persons died, and thousands were displaced (4). The international community responded to these events with the largest relief measures ever undertaken for a natural disaster (5). To determine the health and nutrition status of the affected populations and to evaluate the effectiveness of relief interventions 7 months after the tsunami and 3 months after the second earthquake, Cooperative for Assistance and Relief Everywhere, Inc. (CARE) International Indonesia and CDC conducted surveys in three districts of Aceh Province (Aceh Besar, Banda Aceh, and Simeulue) (Figure). This report summarizes the results of those surveys, which identified routine vaccinations and provision of toilets or latrines as particular areas for improvement and revealed no significant difference in health indicators between internally displaced persons (IDPs) and nondisplaced populations. The relief response in Aceh Province should target areas needing improvement with programs that serve both IDPs and nondisplaced persons, as measures are implemented to rebuild the public health infrastructure. Three separate, two-stage, random-cluster surveys (6) were conducted during July--August 2005 among households in the three districts. Both Aceh Besar (estimated 2005 population: 295,000) and Banda Aceh (178,000) were severely affected by the first earthquake and tsunami; Simeulue (78,000) was affected primarily by the second earthquake (2). Interviewers used hand-held computers to administer questionnaires, and informed consent was obtained from all participants. The height and weight of children aged 6--59 months were measured; finger-stick blood samples for evaluation of anemia and malaria and stool samples were obtained for detection of soil-transmitted helminths were obtained from every second child aged 6--59 months. Among children in this age group, 17% did not complete anthropometric and laboratory assessment. Differences in proportions between IDPs and nondisplaced persons were tested using chi-square tests with a statistical significance level of p<0.05; confidence intervals were calculated using statistical software to accommodate the complex sampling design. A total of 2,751 households were in the initial sampling; residents of 101 (3.7%) households either refused to participate or did not complete the questionnaire, leaving 2,650 households in the three surveys. Average household size was 5.2 persons. Of 13,712 persons in the households surveyed, 51.4% were male and 11.3% were children aged <5 years. At the time of the survey, the highest proportion of displaced households was in Simeulue (32.3%), followed by Aceh Besar (22.4%) and Banda Aceh (15.8%) (Table 1). Interviewed IDPs either were housed in camps or had found shelter with other families. Persons in an additional 46% of households in the three districts had been temporarily displaced but had returned to their residences. The highest proportion of households with partial or complete damage to homes was in Simeulue, where 82.3% of homes were affected, followed by 61.8% in Banda Aceh and 47.3% in Aceh Besar (Table 1). Limited numbers of households with damaged homes had received building materials for reconstruction (11.4% in Aceh Besar, 3.1% in Banda Aceh, and 2.4% in Simeulue). Plastic sheeting for temporary shelter had been received by 82.5% of households with damaged houses in Simeulue, 27.7% in Aceh Besar, and 20.9% in Banda Aceh. Food assistance (e.g., rice, noodles, fish, and oil) had been received by 90.4% of households in Simeulue, 62.2% in Banda Aceh, and 41.6% in Aceh Besar. Among children aged 12--59 months, distribution of micronutrient supplements was highest in Simeulue (60.8% among IDPs and 53.2% among nondisplaced children), lowest in Banda Aceh (25.0% among IDPs and 15.1% among nondisplaced children), and significantly lower among nondisplaced children (22.7%) than IDPs (55.9%) in Aceh Besar (Table 2). Among children aged 6--59 months, global acute malnutrition (GAM) (7) ranged from 7.8% among nondisplaced children in Banda Aceh to 17.6% among IDPs in Simeulue. Severe acute malnutrition (SAM) was highest in Simeulue (3.4% among IDPs and 1.9% among nondisplaced children) (Table 2). GAM was not significantly higher among IDPs in the three districts, and no association was observed between food aid distribution and GAM. A measles vaccination campaign targeted all children aged 6 months--15 years. Among eligible children aged 12--59 months, the percentage receiving measles vaccination ranged from 37.3% of IDPs in Aceh Besar to 58.2% of nondisplaced children in Banda Aceh (Table 2). Among children in this age group, the key point of contact for Indonesian public health services, including routine vaccination, is a monthly growth-monitoring service called the Posyandu. Approximately half of all children surveyed in this age group had been evaluated by the Posyandu during the preceding 3 months. In the three districts, mild or moderate anemia among children aged 6--59 months ranged from 31.8% to 64.5% (Table 2). The prevalence of anemia among IDPs did not differ significantly from that of nondisplaced children. Soil-transmitted helminth infections, primarily ascariasis and trichuriasis, were common among children in Aceh Besar and Simeulue, where approximately 75% of school-aged children and half of children aged 6--59 months were infected. Prevalence of helminth infection was significantly lower (p<0.05) among children in Banda Aceh than among children in the other two districts. Nearly 80% of displaced households in urban Banda Aceh and Aceh Besar had access to a protected source of drinking water (i.e., bottled, municipal tap, tanker-delivered, or deep borehole). By contrast, in Simeulue, a rural district that is poorer and more isolated, 18% had access to a protected water source, with most families collecting water from shallow wells or surface-water sources. Access to a protected water source was significantly higher (p<0.05) among IDPs (76.7%) than among nondisplaced persons (30.5%) in Aceh Besar (Table 2). Overall, boiling of drinking water was reported by 84% of households, regardless of the water source. However, 40% of samples of stored drinking water (21.3% in Banda Aceh, 45.7% in Aceh Besar, and 52.5% in Simeulue) tested positive for Escherichia coli, suggesting poor water handling and storage practices. Among households in Aceh Besar and Banda Aceh, respectively, 77% and 98% had access to toilets or latrines. However, in Simeulue, access to toilets or latrines remained limited (45.5% among IDP households and 60.1% among nondisplaced households). Approximately 93% of households in Simeulue used bed nets as protection from mosquitoes, compared with approximately 36% of households in urban Banda Aceh (Table 2). In Aceh Besar, use of bed nets was significantly higher (p<0.05) among IDP households (80.8%) than among nondisplaced households (52.2%). Indoor residual spraying for mosquitoes also was higher among IDP households (65.3%) in Simeulue but lower among IDP households (13.2%) in Banda Aceh. Reported by: E Widyastuti, MD, G Silaen, MD, A Pricesca, MD, A Handoko, CARE International, Indonesia. C Blanton, MS, T Handzel, PhD, M Brennan, MD, Div of Emergency and Environmental Health Sciences, National Center for Environmental Health; O Mach, MD, EIS Officer, CDC. Editorial Note:Before the December 2004 tsunami, Aceh Province was isolated by ongoing civil conflict. After the tsunami, unprecedented measures by local and international agencies were taken to provide temporary shelter, food, and drinking water. An early warning disease surveillance system was implemented, and a mass measles vaccination campaign, together with administration of vitamin A, was initiated as a collaborative program of the Indonesian government, World Health Organization (WHO), UNICEF, and other nongovernmental organizations (8). No large disease outbreaks were reported during the relief period, and mortality from disease was low. The surveys and measurements described in this report, conducted 7 months after the tsunami and 3 months after the second earthquake, observed levels of malnutrition similar to those identified by earlier surveys conducted in the same districts during February--March 2005 (UNICEF, unpublished data, 2005), suggesting food conditions were stable. Malnutrition levels were below the WHO emergency threshold for GAM of 15% (7) in Banda Aceh and Aceh Besar but were elevated in Simeulue. However, this finding might reflect high rates of malnutrition in Simeulue before the earthquake. The results also indicate that food and drinking water were provided to the majority of the population, although improvements to prevent contamination of drinking water were needed. Despite these successes, substantial gaps in the relief program remained. Both measles vaccination coverage and micronutrient supplement coverage were low. Access to basic sanitation was deficient in rural areas such as Simeulue. One half of children aged <5 years were anemic. Nearly one half of preschool children and three fourths of school-aged children were infected with soil-transmitted helminths in Aceh Besar and Simeulue. In general, health indicators were similar among IDPs and nondisplaced populations, warranting relief strategies that provide assistance to both populations in Aceh Province. Data from these and other surveys in Aceh Province are being used to plan longer-term health and nutrition interventions. In Simeulue, for example, local government and nongovernmental organizations are strengthening the growth-monitoring system. This will improve vaccination coverage, micronutrient supplementation, and access to feeding programs for malnourished children. Measles and deworming campaigns will be conducted in Aceh Province. These and other programs, such as construction of water and sanitation infrastructure, will benefit both IDPs and nondisplaced populations. The findings in this report are subject to at least two limitations. First, results from the three districts might not be representative of all areas of Aceh Province affected by the tsunami and second earthquake. Second, because only limited data were available regarding the health and nutrition status of the populations in these districts before the tsunami, determining to what extent the findings on health indicators reflect underlying conditions or the effects of the disaster and subsequent displacement was not possible. With improved access to formerly isolated areas of Aceh Province and recovery resources made available, expectations for the humanitarian response are high. In addition to rebuilding homes, an opportunity exists to rebuild the public health infrastructure in the province. Monitoring health and nutrition indicators can continue to ensure that standards for relief measures are met by international agencies and nongovernmental organizations. Acknowledgments This report is based, in part, on assistance provided by M Yulizar, MD, Provincial Health Office, Aceh, Indonesia; A Kurniawan, MD, Directorate of Community Nutrition, Ministry of Health, Indonesia; and J Vanden Eng, MPH, MS, and A Wolkon, MPH, Division of Parasitic Diseases, National Center for Infectious Diseases, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/2/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|