|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
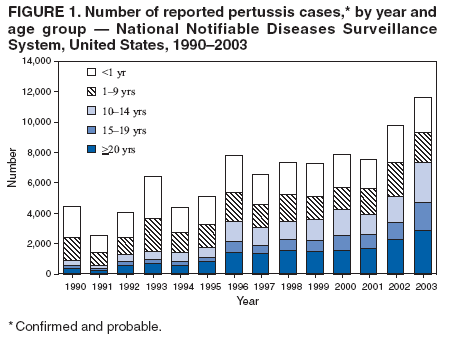
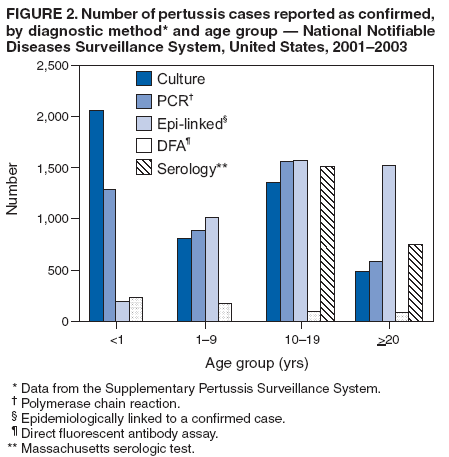
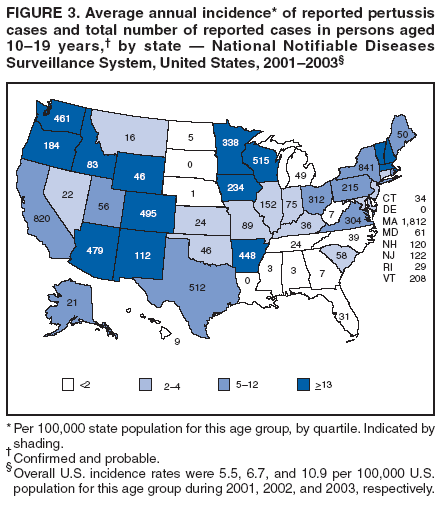
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Pertussis --- United States, 2001--2003Pertussis is a highly contagious, vaccine-preventable bacterial illness characterized by paroxysmal cough, posttussive vomiting, and inspiratory whoop. Pertussis also can occur as a mild or moderate cough illness in persons who are partially immune (1). In the United States, most hospitalizations and nearly all deaths from pertussis are reported in infants aged <6 months, but substantial morbidity does occur in other age groups. Infant/childhood vaccination has contributed to a reduction of more than 90% in pertussis-related morbidity and mortality since the early 1940s in the United States (1). Estimates of childhood vaccination coverage with >3 doses of pertussis-containing vaccine have exceeded 90% since 1994; however, reported pertussis cases increased from a historic low of 1,010 in 1976 to 11,647 cases in 2003 (2). A substantial increase in reported cases has occurred among adolescents, who become susceptible to pertussis approximately 6--10 years after childhood vaccination (3,4). Recently, booster vaccines for adolescents and adults combining pertussis antigens with tetanus and diphtheria toxoids (Tdap) were approved by the Food and Drug Administration (FDA).* On June 30, 2005, the Advisory Committee on Immunization Practices (ACIP) recommended Tdap for all persons aged 11--18 years. This report summarizes national surveillance data on pertussis reported to CDC during 2001--2003 and focuses on pertussis reported among persons aged 10--19 years before implementation of national recommendations for adolescent pertussis vaccination. Pertussis cases are reported weekly by state health departments to CDC through the National Notifiable Diseases Surveillance System (NNDSS); more detailed information about cases is provided through the linked Supplementary Pertussis Surveillance System (SPSS). Probable and confirmed cases are reported; however, six states do not report probable cases. A clinical case is defined as an acute cough illness lasting >14 days in a person with at least one symptom characteristic of pertussis (i.e., paroxysmal cough, posttussive vomiting, or inspiratory whoop) or >14 days of cough in an outbreak setting. A confirmed case is defined as 1) a cough illness of any duration with isolation by culture of Bordetella pertussis or 2) a case that is consistent with the clinical case definition and is confirmed by polymerase chain reaction (PCR) testing or epidemiologic linkage to a laboratory-confirmed case. In addition, Massachusetts uses an in-state, standardized serologic assay for persons aged >11 years as a confirmatory test. A probable case is defined as a case that is consistent with the clinical case definition but does not have laboratory confirmation or an epidemiologic link. Direct fluorescent antibody (DFA) assays are no longer recommended for pertussis testing; however, cases continue to be reported as confirmed by DFA. For this report, age-specific and race-specific incidence rates were calculated using U.S. Census Bureau population estimates for 2001--2003. During 2001--2003, a total of 28,998 cases of pertussis were reported to NNDSS from the 50 states and the District of Columbia (7,580 in 2001; 9,771 in 2002; and 11,647 in 2003); 69% of these cases were reported as confirmed. Among all pertussis cases, 15,620 (54%) were in females. Overall in the United States, the average annual incidence was 3.3 cases per 100,000 population (2.7 in 2001, 3.4 in 2002, and 4.0 in 2003). Among 28,923 (99.7%) persons with pertussis for whom age was reported, 6,608 (23%) were aged <1 year (including 5,872 aged <6 months), 3,353 (12%) were aged 1--4 years, 2,553 (9%) were aged 5--9 years, 9,609 (33%) were aged 10--19 years, and 6,800 (23%) were aged >20 years (Figure 1). By age group, average annual incidence was highest (55.2 per 100,000 population) among infants aged <1 year; within that group, incidence was 98.2 for infants aged <6 months and 12.3 for infants aged 6--11 months. Incidence was lower for older groups: 7.2 per 100,000 population for children aged 1--4 years, 4.3 for children aged 5--9 years, 7.7 for persons aged 10--19 years, and 1.1 for adults aged >20 years. During 2001--2003, the annual incidence of pertussis among persons aged 10--19 years increased from 5.5 per 100,000 in 2001, to 6.7 in 2002, and 10.9 in 2003. Race and Hispanic ethnicity were considered independently. Data on race were available for 24,024 (83%) persons with pertussis. Of these, 21,597 (90%) were white, 1,621 (7%) were black, 288 (1%) were American Indian/Alaska Native, 337 (1%) were Asian/Pacific Islander, and 181 (1%) were identified as "other race." Among the 7,991 (83%) persons aged 10--19 years whose race was reported, 7,549 (95%) were white and 265 (3%) were black. Among all age groups, the incidence of reported cases was twice as high among whites as among blacks (3.0 versus 1.4 cases per 100,000 population). After stratifying by state, the white-to-black incidence rate ratio was 1.6. Data on Hispanic ethnicity were available for 23,669 (82%) persons with pertussis. Of these, 3,871 (16%) were Hispanic. Among infants aged <6 months, 1,701 (29%) of 5,872 with pertussis were Hispanic; by comparison, an estimated 18% of infants born each year in the United States are Hispanic. Of 9,609 persons aged 10--19 years with reported pertussis, 116 (1%) of 8,286 for whom information was provided were hospitalized, 148 (2%) of 7,560 had radiographically confirmed pneumonia, and 20 (0.2%) of 8,543 reported seizures as a complication of pertussis. Hospitalization and complications of pertussis were most common among infants aged <6 months. Of the total 5,872 infants aged <6 months, 3,255 (69%) of 4,748 for whom information was provided were hospitalized, 532 (13%) of 4,096 had radiographically confirmed pneumonia, and 79 (2%) of 4,802 had seizures. Among persons of all ages with pertussis, 33 cases of encephalopathy and 56 pertussis-related deaths were reported during 2001--2003. Fifty-one (91%) of the deaths were among infants aged <6 months, and 42 (75%) of the deaths were among infants aged <2 months. Compared with other age groups, the greatest number of reported cases was among persons aged 10--19 years. Among the 6,090 (63%) of 9,609 persons in this age group reported as having confirmed pertussis, 1,570 cases (26%) were confirmed by an epidemiologic link to a confirmed case, 1,356 (22%) by culture, 1,562 (26%) by PCR, and 1,511 (25%) by the Massachusetts serologic test (Figure 2). Massachusetts alone reported 1,812 cases, accounting for 19% of the total U.S. cases in persons aged 10--19 years; by comparison, Massachusetts has 2% of the U.S. population aged 10--19 years. Massachusetts had the highest state average annual incidence in this age group (78.8 per 100,000 population); the median state average annual incidence for this age group was 3.7 per 100,000 population (range: 0--78.8) (Figure 3). Reported by: K Brown, MM Cortese, MD, K Iqbal, MPH, JS Moran, MD, TV Murphy, MD, VP Sneller, PhD, P Srivastava, MPH, Epidemiology and Surveillance Div, National Immunization Program; AC Cohn, MD, EIS Officer, CDC. Editorial Note:Reported cases of pertussis in the United States have increased since 1976, with a substantial increase among persons aged 10--19 years (5). Compared with the increase observed in reported cases among adolescents, the increases in cases reported in age groups that contain recently vaccinated children have been small (5,6). Compared with older age groups, infants aged <6 months continued to have the highest reported incidence of pertussis, and Hispanic infants were overrepresented in this group, as also demonstrated in a previous study (7). Among all age groups, the reported pertussis incidence in whites was higher than the incidence in blacks. However, passive surveillance probably does not equally reflect the relative burden of pertussis in all racial and ethnic groups; even among reported cases, race and ethnicity data were complete in only 74% of cases. How much the increase in reported cases of pertussis in adolescents reflects a true change in the burden of disease remains unclear. Better recognition, diagnosis, and reporting of pertussis in persons aged 10--19 years likely has contributed to the greater number of cases reported. Although the Council of State and Territorial Epidemiologists has made no changes to the case definition for pertussis since 1996 (when PCR was added as a confirmatory test for cases that also are consistent with the clinical case definition), an increasing number of states now use PCR for confirmatory testing. In addition, heightened recognition of pertussis transmitted in schools and other settings likely adds to the number of cases detected and reported among persons aged 10--19 years. Wide variability was observed in incidence of cases reported by individual states. Massachusetts, for example, has long reported higher incidence in adolescents compared with other states, and Massachusetts data are believed to more closely reflect the pertussis burden in U.S. adolescents (8). These results from Massachusetts have been obtained, in part, through the state's enhanced pertussis surveillance among students in middle and high school and through development and availability of a serologic test for pertussis in persons aged >11 years. Awareness of pertussis in adolescents, however, is still low in many places, as suggested in part by eight states reporting an average annual incidence of <1 case per 100,000 persons aged 10--19 years during the 3-year period. A population-based, active surveillance study during 1995--1996 estimated pertussis incidence at 507 per 100,000 population aged 10--49 years, demonstrating that passive pertussis surveillance is capturing only a fraction of cases among older persons (9). Diagnostic testing for pertussis remains inadequate for surveillance and clinical management. Culture is specific but not sensitive. PCR is likely more sensitive, but no FDA-licensed test kit is available and no nationally accepted standardized protocol for test performance exists. Most laboratory validation studies have not sufficiently established the predictive value of a positive PCR test in cases of pertussis; the rate of false-positive tests varies from laboratory to laboratory (10). PCR-confirmed cases contribute a substantial proportion of the total reported cases among persons aged 10--19 years. Moreover, many cases confirmed by epidemiologic linkage to laboratory-confirmed cases are linked to PCR-confirmed cases, potentially multiplying the contribution of PCR testing to the overall number of cases reported. Cases that are PCR positive should be reported only if they also meet the clinical case definition criteria. DFA is neither specific nor sensitive and is no longer recommended for pertussis testing; nonetheless, 2% of cases were reported as DFA-confirmed. Implementing the ACIP recommendation to vaccinate persons aged 11--18 years with Tdap should substantially reduce morbidity associated with pertussis among adolescents. In addition, the cost of case investigations and outbreak-control measures by local and state health departments likely will be reduced by an effective vaccination program targeting persons aged 11--18 years. Ensuring high coverage with Tdap in adolescents is an important step to better control pertussis in the United States. Acknowledgment The findings in this report are based, in part, on data contributed by state and local health departments. References
* BOOSTRIX® (GlaxoSmithKline Biologicals, Rixensart, Belgium) was licensed May 3, 2005, for use in persons aged 10--18 years, and ADACELTM (Sanofi Pasteur, Toronto, Canada) was licensed June 10, 2005, for use in persons aged 11--64 years.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 12/21/2005 |
|||||||||
|