|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
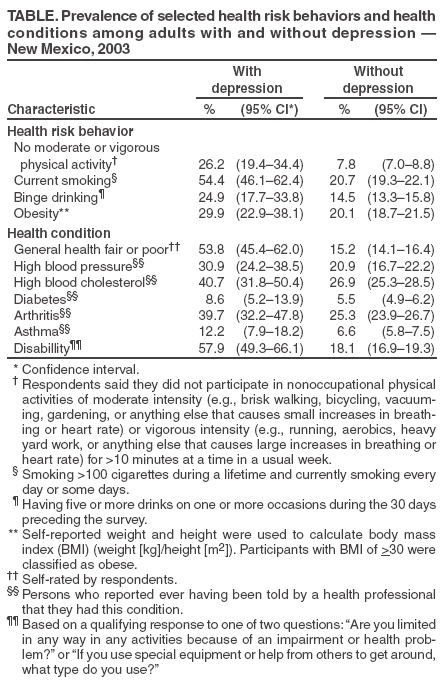
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Mental Health in the United States: Health Risk Behaviors and Conditions Among Persons with Depression --- New Mexico, 2003Studies have demonstrated relationships between physical health and mental health (1,2). Chronic disease has been associated with depression, which, in the absence of intervention, also can assume a chronic course (3). To determine the prevalence of depression among adults in New Mexico and examine the association between depression and selected health risk behaviors and health conditions, the New Mexico Department of Health and CDC analyzed data from the 2003 New Mexico Behavioral Risk Factor Surveillance System (BRFSS) survey. This report describes the results of that analysis, which determined that 3.8% of adults in New Mexico had current symptoms of depression and that these adults were significantly more likely to have engaged in certain health risk behaviors (e.g., smoking and binge drinking) and to have certain health conditions (e.g., high blood pressure, high blood cholesterol, arthritis, and asthma) than persons without depression. Public health programs that promote mental health and timely diagnosis and treatment of depression might also help reduce morbidity and risk behaviors related to chronic diseases. New Mexico BRFSS is a state-based component of the CDC BRFSS, through which states conduct random-digit--dialed telephone surveys of their noninstitutionalized, civilian population aged >18 years. In 2003, a total of 5,494 adults participated in the New Mexico survey; the CASRO response rate was 56.4%. The New Mexico survey included six questions adapted from the Primary Care Evaluation of Mental Disorders (PRIME-MD) to assess the prevalence of depression among adults in the state. Two screening questions were asked: "During the past 30 days, have you often been bothered by feeling down, depressed, or hopeless?" and "During the past 30 days, have you often been bothered by little interest or pleasure in doing things?" (4). Respondents who answered "yes" to either screening question were then asked the other four core depressive symptom questions. Respondents were asked how often during the preceding 14 days they had been "bothered by little interest or pleasure in doing things," "bothered by trouble falling or staying asleep, or sleeping too much," "bothered by poor appetite or overeating," and "bothered by feeling bad about yourself, or that you are a failure or have let yourself or your family down" (5). Participants chose from the following four responses: "not at all," "several days," "more than half of the days," and "nearly every day." Respondents were considered depressed if they answered "yes" to either of the two PRIME-MD screening questions and "nearly every day" to two or more of the four questions regarding depressive symptoms (4). Data were weighted to reflect the demographic profile of the noninstitutionalized civilian population of New Mexico. Differences in point estimates were considered not significant if their 95% confidence intervals (CIs) overlapped. The overall prevalence of depression among adults in New Mexico was 3.8% (CI = 3.2%--4.5%) and varied significantly by age, race/ethnicity, income, and education but not by sex. Results of age-group analysis indicated that persons aged 45--54 years (4.9%; CI = 3.4%--6.8%) were most likely to be depressed and that those aged >75 years (1.7%; CI = 0.9%--3.2%) were least likely to be depressed. Among racial/ethnic groups, prevalence of depression ranged from 4.9% (CI = 3.8%--6.1%) among Hispanics to 1.8% (CI = 0.6%--5.2%) among American Indians/Alaska Natives. By income, persons with annual household incomes of <$10,000 had the highest prevalence of depression (12.7%; CI = 8.6%--18.4%), and those with incomes of >$50,000 had the lowest prevalence (1.4%; CI = 0.9%--2.2%). By education level, adults who had not graduated from high school had the highest prevalence of depression (7.8%; CI = 5.6%--11.0%), and those who had graduated from college had the lowest prevalence (1.7%; CI = 1.1%--2.5%). Adults with depression were significantly more likely than those without depression to report the following health risk behaviors or health conditions*: fair or poor general health (53.8% versus 15.2%), no moderate or vigorous physical activity (26.2% versus 7.8%), current smoking (54.4% versus 20.7%), binge drinking (24.9% versus 14.5%), obesity (29.9% versus 20.1%), high blood pressure (30.9% versus 20.9%), and high blood cholesterol (40.7% versus 26.9%). However, no significant difference was determined for those with or without diabetes (Table). Reported by: J Daniel, MPH, W Honey, MPH, M Landen, MD, New Mexico Dept of Health. S Marshall-Williams, PhD, D Chapman, PhD, J Lando, MD, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that, in New Mexico, certain adverse health risk behaviors and health conditions are more common among persons with depression than among persons without depression, underscoring the importance of considering mental health in the prevention and treatment of chronic illnesses. Among the risk behaviors and conditions considered, the findings from this study did not indicate a significant relationship between diabetes and depression, which is consistent with the results of a previous study (6) but inconsistent with the results of another (7). In addition, the overall estimated 3.8% prevalence of depression is lower than the 6.7% prevalence estimated by the U.S. National Comorbidity Survey Replication. However, the prevalence in this report was based on telephone interviews with participants regarding depressive symptoms that occurred during the preceding 14 days; the national comorbidity survey prevalence came from symptoms that occurred during a 12-month period, based on face-to-face interviews conducted during 2001--2003 (8). The findings in this report are subject to at least four limitations. First, the data on which they were based were self-reported by telephone survey and might have been different had they been obtained by physical and psychiatric examination. Second, data were collected only from noninstititutionalized adult residents with landline telephones; these data might not be generalizable to persons in younger age groups, who might be more likely to use cellular phones exclusively. Third, only residents of New Mexico were surveyed, and results might not be generalizable to persons residing in other regions of the United States. Finally, because these data are cross-sectional, they do not permit any inference of a causal pathway between depression and the physical health risk behaviors and health conditions investigated. Nonetheless, the findings in this report corroborate the correlation between depression and chronic diseases and conditions determined by previous studies (3) and thus suggest that the assessment and treatment of depression can help to improve the overall health of a population. Although depressive disorders can be treated successfully, data ranging from the Epidemiologic Catchment Area program in the early 1980s to those collected by the 2002 National Health Interview Survey indicated that most persons needing treatment for mental illness did not receive treatment (9). Barriers to treatment include the stigma associated with depression, lack of knowledge about depression, and lack of adequate insurance coverage (2). Persons with depression, particularly those who also have a physical health condition, might seek treatment from various types of health-care professionals (e.g., general practitioners) other than psychiatrists, psychologists, or psychiatric social workers. The U.S. Preventive Services Task Force (USPSTF) recommends screening adults for depression in clinical practices if systems exist to ensure accurate diagnosis, effective treatment, and follow-up. USPSTF determined that screening increases the accurate identification of depressed patients in primary-care settings and that treatment of depressed adults in primary-care settings decreases their level of clinical morbidity (10). CDC can help increase understanding of depression and its public health burden by conducting mental health surveillance and working with national partners, such as the National Mental Health Association, Substance Abuse and Mental Health Services Administration, and National Institute of Mental Health to address the prevention and treatment of mental illnesses. New Mexico plans to continue its population-based surveillance for depression through BRFSS. References
* Fair or poor general health: Self-rated by respondents. No moderate or vigorous physical activity: Respondents said they did not participate in nonoccupational physical activities of moderate intensity (e.g., brisk walking, bicycling, vacuuming, gardening, or anything else that causes small increases in breathing or heart rate) or vigorous intensity (e.g., running, aerobics, heavy yard work, or anything else that causes large increases in breathing or heart rate) for >10 minutes at a time in a usual week. Current smoking: >100 cigarettes during a lifetime and currently smoking every day or some days. Binge drinking: Having five or more drinks on one or more occasions during the 30 days preceding the survey. Obesity: Self-reported weight and height were used to calculate body mass index (BMI) (weight [kg]/height [m2]). Participants were classified as obese if their BMI was >30. High blood pressure and high blood cholesterol: Persons reported ever having been told by a health professional that they had these conditions.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/5/2005 |
|||||||||
|