|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
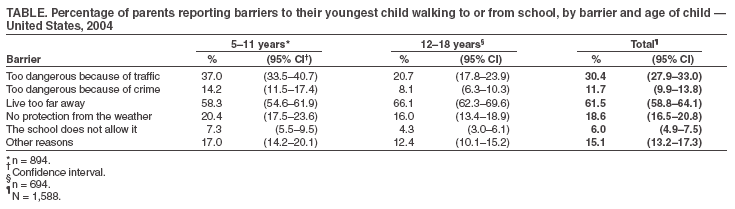
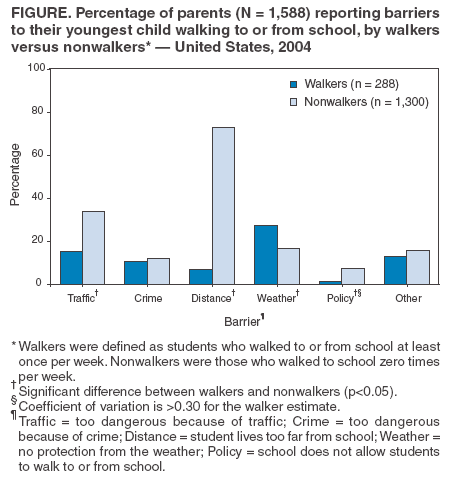
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Barriers to Children Walking to or from School --- United States, 2004Walking for transportation is part of an active lifestyle that is associated with decreased risks for heart disease, diabetes, hypertension, and colon cancer and an increased sense of well being (1). However, the percentage of trips made by walking has declined over time among both children (2) and adults (3). One of the objectives of Healthy People 2010 (no. 22-14b) is to increase among children and adolescents the proportion of trips to school made by walking from 31% to 50% (4). In 1969, approximately half of all schoolchildren walked or bicycled to or from school, and 87% of those living within 1 mile of school walked or bicycled (5). Today, fewer than 15% of children and adolescents use active modes of transportation (2). This report examines data from the 2004 ConsumerStyles Survey and a follow-up recontact survey to describe what parents report as barriers to their children aged 5--18 years walking to or from school. Distance to school was the most commonly reported barrier, followed by traffic-related danger. Comprehensive initiatives that include behavioral, environmental, and policy strategies are needed to address these barriers to increase the percentage of children who walk to school. The ConsumerStyles and recontact surveys are conducted annually by a market-research firm with technical assistance from CDC. For the ConsumerStyles survey, stratified random sampling (by region, household income, population density, age, and household size) was used to identify 10,000 potential respondents from a larger consumer-mail panel of approximately 600,000 adults aged >18 years. A low income/minority supplement and a households-with-children supplement were used to ensure adequate numbers of respondents from those groups. Of the 10,000 identified, 6,207 responded to the initial survey (62% response rate). The recontact survey was mailed to all respondents within 4--6 months of the initial survey and had a 68% response rate (N = 4,213). For that survey, parents of children aged 5--18 years were asked how many times their youngest child walks to or from school during a usual week and whether one or more of six barriers (too dangerous because of traffic, too dangerous because of crime, live too far away, no protection from the weather, the school does not allow it, and other reasons) prevents that child from walking to school. Results were weighted to reflect the age, race/ethnicity, sex, income, and household size of the U.S. adult population, as determined by the 2000 U.S. Census. Of the 1,705 adults who reported having a child aged 5--18 years, 1,588 (93%) answered the walk-to-school questions for their youngest child. Approximately 17% reported that their child walked to or from school at least once per week during a usual week. Among students who walked to school, the average number of trips per week to or from school was 7.1 (range: 1--10). The percentage of students who walked to or from school was higher among those aged 5--11 years than among those aged 12--18 years (18.7% versus 15.3%); this difference was not significant (p = 0.08). The most commonly reported barrier was distance to school (61.5%), followed by traffic-related danger (30.4%), then weather (18.6%). Fifteen percent of parents cited an "other" barrier, 11.7% reported crime as a barrier, and 6.0% reported school policy as a barrier; 15.9% (95% CI = 14.1%--18.0%) of parents selected the response, "It is not difficult for my child to walk to school." The frequency with which barriers were reported by parents varied slightly by age (5--11 years versus 12--18 years), although the relative ranking of the barriers did not differ by age (Table). Barriers also varied by walking status (walker versus nonwalker), with the largest difference observed for distance (72.9% [CI = 70.1%--75.5%] versus 6.8% [CI = 4.5%--10.4%]) (Figure). Reported by: S Martin, S Carlson, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:In this study, distance to school was the most commonly cited barrier to walking to and from school. A similar study conducted in 1999 (6) also found distance to be the most commonly cited barrier (55%). This finding might be attributable, in part, to an increase of 2 million students from 1969 to 2001 with a corresponding decrease in the number of schools, from 70,879 in 1969 to 69,697 in 2001 (7). As a result, a greater percentage of students might live farther than 1 mile from their schools. Study results also indicated that students aged 5--11 years were more likely to walk to school than were those aged 12--18 years; however, this difference was not significant. One possible reason for this difference is that elementary schools are likely to be closer to children's homes because they outnumber junior and senior high schools in the United States (more than 70,000 elementary schools compared with approximately 28,000 junior and senior high schools) (7). This hypothesis is supported by the finding that parents of older children more frequently cited distance as a barrier, whereas parents of younger children more frequently cited other barriers. The findings in this report are subject to at least three limitations. First, the data are subject to sampling biases because data could be collected only from parents who chose to respond to the survey. Second, because the age of each respondent's youngest child was derived from the ConsumerStyles survey, which was mailed 4--6 months earlier, some of the children's ages might have been misclassified. Finally, the survey did not ask parents how far the child lived from school, about whether the child attended a public or private school, or about the presence of sidewalks. Efforts to overcome barriers to walking to school include the nationwide Safe Routes to School (SR2S) initiative, which has received federal and state funding. SR2S programs are designed to increase the percentage of students who walk or bicycle to school by addressing barriers through the "four Es" (engineering, enforcement, education, and encouragement). For example, to address the distance barrier, schools can arrange for children to meet within a mile of school and proceed to school in "walking school buses," in which an adult "driver" and an adult "caboose" escort several children walking together. This strategy might also alleviate fear of crime. To address the traffic barrier, programs might use engineering and enforcement approaches, such as crossing signals (engineering) and better enforcement of speed limits (enforcement). To further allay parental fears of traffic danger, programs might teach children pedestrian skills in the classroom (education). For example, one comprehensive SR2S program in Marin County, California, that uses all of the "four Es" experienced a 64% increase in walking and a 114% increase in bicycling by the second year of their program (8). The SR2S program in Tempe, Arizona, has made engineering improvements to enhance pedestrian safety and has promoted walking through an annual Walk to School Day, in which more than 8,000 students from 20 elementary schools participate. The program has contributed to a decrease in automobile traffic near elementary schools during morning and afternoon rush hours (9). Implementing SR2S programs and removing or alleviating barriers that prevent children from walking to school might foster progress toward achieving the national health objective. Information about programs and resources related to SR2S is available at http://www.cdc.gov/nccdphp/dnpa/kidswalk/index.htm, http://www.walktoschool-usa.org, http://www.walkingschoolbus.org, and http://www.nhtsa.dot.gov/people/injury/pedbimot/bike/safe-routes-2004. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/29/2005
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|