|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
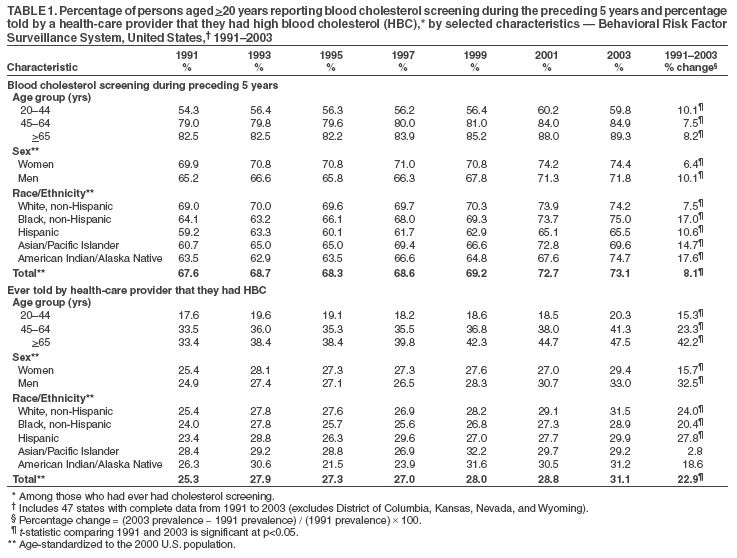
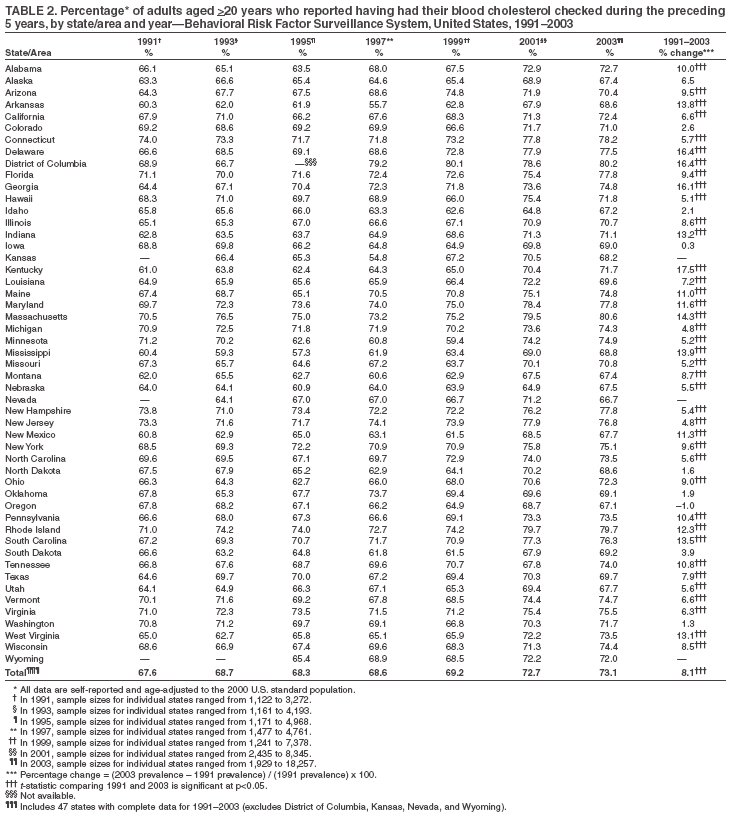
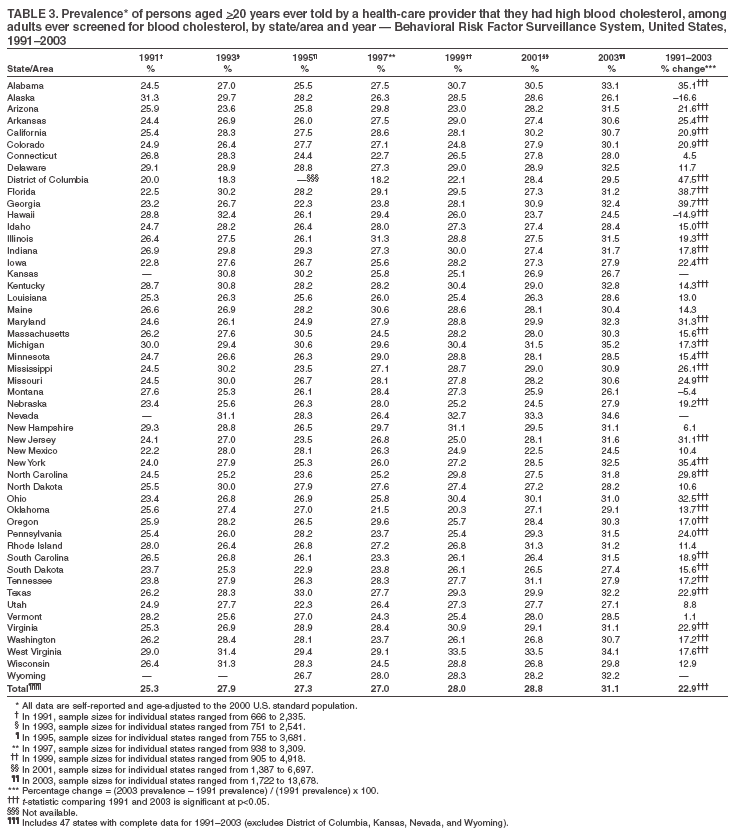
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Trends in Cholesterol Screening and Awareness of High Blood Cholesterol --- United States, 1991--2003High blood cholesterol (HBC) (i.e., total cholesterol >240 mg/dL) is a major risk factor for heart disease, the leading cause of death in the United States (1). As a result, public health agencies and their partners have attempted to reduce the prevalence of HBC through screening and by increasing public awareness of HBC and strategies for reducing it. A national health objectives of Healthy People 2010 is to increase to 80% the proportion of adults aged >20 years who have been screened for HBC within the preceding 5 years (2). For this report, data from the Behavioral Risk Factor Surveillance System (BRFSS) collected during 1991--2003 were analyzed to examine trends in the percentage of adults screened for HBC and the percentage of those screened who were told they had HBC. The findings indicated that both percentages increased during 1991--2003 but that few states had achieved the national health objective for screening. Further emphasis on cholesterol screening is needed, particularly among Hispanic and Asian/Pacific Islander populations and young adults. BRFSS is a state-based, random-digit--dialed telephone surveillance system that samples the noninstitutionalized, U.S. civilian population aged >18 years. For this report, CDC analyzed BRFSS data from 1991, 1993, 1995, 1997, 1999, 2001, and 2003 for 1,027,793 persons aged >20 years. Response rates for BRFSS surveys ranged from 71.4% in 1993 to 51.1% in 2001 (3). Survey participants were asked whether they had ever had a blood cholesterol screening and, if so, how long it had been since their last screening. Those who reported having ever been screened were asked whether they had ever been told by a health-care professional that they had HBC. Data were weighted to account for age, race/ethnicity, and sex distributions of the population in each state. Statistical software was used to account for the complex sampling design. The results were age-standardized to the 2000 U.S. standard population (4). Percentage change was calculated as the 2003 prevalence minus the 1991 prevalence divided by the 1991 prevalence multiplied by 100. During 1991--2003, the prevalence of cholesterol screening during the preceding 5 years and the percentage of persons screened who were told they had HBC increased overall and among all age, sex, and racial/ethnic groups (Table 1). The percentage of those screened within 5 years increased from 67.6% (95% confidence interval [CI] = 67.2--68.1) in 1991 to 73.1% (CI = 72.7--73.4) in 2003. Although the prevalence of cholesterol screening within 5 years was higher among women than men in all years represented, the percentage change in prevalence was smaller for women than men. In 2003, the prevalence of cholesterol screening was lowest among Hispanics (65.5%; CI = 64.1--67.0) and Asians/Pacific Islanders (69.6%; CI = 66.9--72.4). The largest percentage changes in prevalence of cholesterol screening were among American Indians/Alaska Natives and non-Hispanic blacks. The overall percentage of those screened who had been told they had HBC increased from 25.3% (CI = 24.7--25.8) in 1991 to 31.1% (CI = 30.7--31.5) in 2003. The percentage change among men told they had HBC was more than twice that among women. The percentage of those screened who were told they had HBC was higher in all racial/ethnic groups in 2003 than in 1991, with the greatest increase observed among Hispanics. Similarly, reporting of HBC increased among all age groups, with the largest percentage change in prevalence among those aged >65 years. In 46 states and the District of Columbia (DC), the prevalence of screening increased from 1991 to 2003, with percentage change ranging from 0.3% in Iowa to 17.5% in Kentucky (Table 2). However, by 2003, only DC and Massachusetts had achieved the Healthy People 2010 objective for cholesterol screening, with rates of 80.2% and 80.6%, respectively. The proportion of screened adults who had been told they had HBC increased in 44 states and DC, with increases ranging from 1.1% in Vermont to 47.5% in DC (Table 3). Reported by: AE Saddlemire, CH Denny, PhD, KJ Greenlund, PhD, JN Coolidge, MPH, AZ Fan, MD, PhD, JB Croft, PhD, Div for Heart Disease and Stroke Prevention, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that the overall percentage of adults who had had their cholesterol checked during the preceding 5 years increased during 1991--2003. However, in most states, increases in screening were moderate; by 2003, only DC and Massachusetts had achieved the Healthy People 2010 objective of 80% screening prevalence. Among those persons who had ever undergone cholesterol screening, the percentage told that they had HBC also increased during 1991--2003. The largest increase in the prevalence of HBC screening occurred during 1999--2001 (5.1%), and in most states, the prevalence of screening continued to increase during 2001--2003. The overall increase in cholesterol screening might have been attributable, in part, to 1) implementation of state heart-disease and stroke-prevention programs by CDC beginning in 1998 (5); 2) release, in 2000, of Healthy People 2010, with the objective to increase the proportion of adults who have had their blood cholesterol checked during the preceding 5 years (2); and 3) publication of the National Cholesterol Education Program Adult Treatment Panel (ATP) II (1993) and ATP III (2001) reports, which updated clinical guidelines for cholesterol testing and management (6,7). In addition, the large increase in prevalence of screening among American Indians/Alaska Natives might be the result of a campaign by the Indian Health Service to improve cholesterol screening, particularly among persons at high risk for cardiovascular disease, including those with diabetes (JM Galloway, MD, Indian Health Service, personal communication, 2004). The increase in percentage of persons ever screened who were told that they had HBC might reflect either an increased prevalence of cholesterol screening or an increase in the prevalence of HBC in the population. However, data based on actual serum cholesterol levels indicate that the percentage of the U.S. population aged >20 years with HBC decreased slightly between the 1988--1994 and 1999--2002 National Health and Nutrition Examination Surveys (8). The findings in this report are subject to at least two limitations. First, BRFSS data are based on respondent self-reports; respondents might have been unaware, forgotten, or not been told that they had been screened for cholesterol or had HBC, resulting in an underestimation of the prevalence of screening and HBC. Second, BRFSS excludes households without telephones. HBC is one of the major modifiable risk factors for heart disease and stroke. One approach to reducing blood cholesterol levels has been to increase public awareness and reinforce educational messages about the risks of HBC (5,6,9). Cholesterol levels can be reduced through dietary changes (e.g., reduced intake of saturated fats and dietary cholesterol), increased physical activity, and drug treatment (7). Although substantial progress has been made in reducing cholesterol levels since the mid-1980s (9), an increased emphasis on cholesterol screening is necessary if more states are to achieve objectives set forth in Healthy People 2010. The public health community and health-care systems should emphasize cholesterol screening of young adults and Hispanic and Asian/Pacific Islander populations to meet the national health objective and the overall Healthy People 2010 goal of eliminating health disparities. Acknowledgment This report is based, in part, on contributions by A Tsai, PhD, Minnesota Dept of Health. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/7/2005
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|