|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
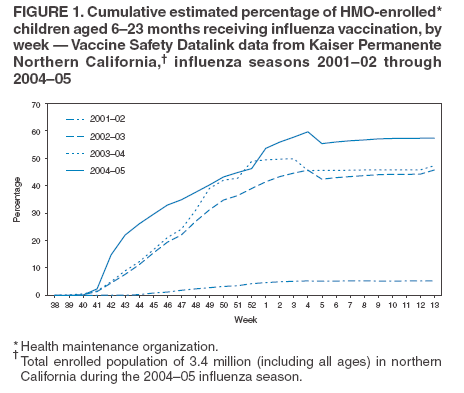
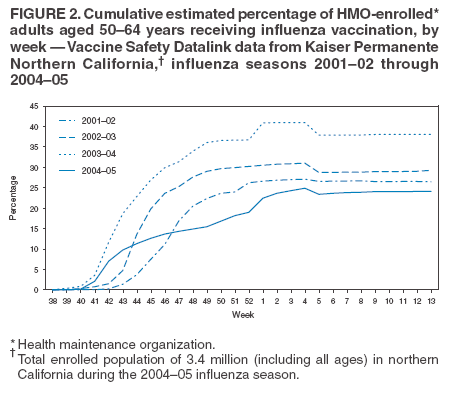
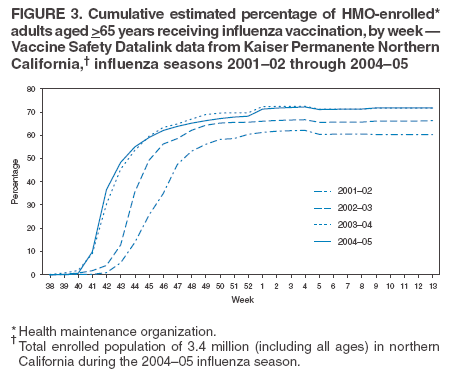
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Rapid Assessment of Influenza Vaccination Coverage Among HMO Members --- Northern California Influenza Seasons, 2001--02 Through 2004--05The Vaccine Safety Datalink (VSD) is a collaborative project involving CDC and eight health maintenance organizations* (HMOs) in the United States. Computerized data on vaccination, medical outcomes, and patient demographics are collected and linked under a standard protocol at multiple HMOs (1). Beginning with the 2003--04 influenza season, the VSD team and one of the HMOs, Kaiser Permanente Northern California (KPNC), established an automated system for rapid detection of potentially adverse events after vaccinations among its members. During the 2004--05 influenza season, in response to the influenza vaccine shortfall and resulting prioritization of vaccine distribution (2), this rapid analysis system also was used to assess influenza vaccination coverage weekly among KPNC members. The results indicated that KPNC followed Advisory Committee on Immunization Practices (ACIP) prioritization guidelines by targeting influenza vaccination to children aged 6--23 months and adults aged >65 years. For the 2005--06 influenza season, the rapid analysis system should be expanded to include data from additional HMOs and more detailed information on vaccinees (e.g., high risk for influenza complications [3]) to better characterize influenza vaccination coverage during the 2005--06 influenza season on a weekly basis. During the 2004--05 influenza season, KPNC had an enrolled population of approximately 3.4 million and received approximately 50% of the influenza vaccine doses it had ordered. By using the KPNC rapid analysis system, the VSD team prospectively assessed weekly influenza vaccination coverage in five age groups (6--23 months, 2--17 years, 18--49 years, 50--64 years, and >65 years) for the 2004--05 influenza season. Beginning in October 2004, KPNC provided weekly counts of influenza vaccinations, stratified by age group, from its immunization registry, which tracks 98.7% of KPNC vaccinations. These data were transmitted to CDC via a secure system. By analyzing estimates of weekly KPNC enrollments and exact vaccination counts, VSD was able to provide weekly estimates of influenza vaccination coverage among the five KPNC age groups. For influenza seasons before 2004--05, the VSD team obtained monthly estimates of total KPNC enrollment for each age group from existing VSD annual data and retrospectively estimated weekly vaccination coverage among KPNC enrollees. However, for the weekly analysis of 2004--05 data, current enrollment estimates by age group were not available; therefore, monthly KPNC enrollment figures from 2003 were used as a proxy for 2004--05 enrollment. A previous sensitivity analysis of this technique for the 2002--03 influenza season determined that estimates of vaccination coverage differed by a range of 0.5% to 3.1% by week and age group when using 2001--02 enrollment as a proxy for the 2002--03 enrollment. To be counted as enrolled for a given month, a person had to be enrolled for the entire month; age for each enrollee was measured from the start of each month of interest. Monthly enrollment estimates were then used to impute corresponding weekly enrollment numbers. Among KPNC members, influenza vaccination coverage levels for the 2004--05 influenza season were 57.4% (95% confidence interval [CI] = 56.9%--57.8%) for children aged 6--23 months (Figure 1), 6.6% (CI = 6.6%--6.7%) for children aged 2--17 years, 6.0% (CI = 5.9%--6.1%) for adults aged 18--49 years, 24.1% (CI = 24.0%--24.2%) for adults aged 50--64 years (Figure 2), and 71.8% (CI = 71.6%--71.9%) for adults aged >65 years (Figure 3). Among two priority groups for influenza vaccination during the 2004--05 influenza season, coverage for children aged 6--23 months was 21.4% greater than the final estimate (47.3%) for the 2003--04 season (Figure 1), and coverage for adults aged >65 years was similar to that for the 2003--04 season (71.7%) (Figure 3). For the remaining age groups, including adults aged 50--64 years (Figure 2), coverage estimates were all significantly less than (p<0.05) final coverage estimates for the previous two influenza seasons. Reported by: N Lewis, S Black, MD, Kaiser Permanente Northern California, Oakland, California. E Weintraub, MPH, J Baggs, PhD, W Thompson, PhD, F DeStefano, MD, R Davis, MD, Immunization Safety Office; D Shay, MD, National Center for Infectious Diseases, CDC. Editorial Note:During the 2004--05 influenza season, when vaccine supply was limited, KPNC influenza-vaccination outreach and communication programs for members were targeted to groups at high risk for influenza complications, in accordance with ACIP recommendations (2,4). As measured by KPNC's new rapid analysis system, vaccination coverage among its members was greater than or similar to that of previous seasons for the two priority age groups, children aged 6--23 months and adults aged >65 years. Vaccination coverage for the nonpriority age groups was significantly lower than that for previous years. These results indicate that KPNC was successful in distributing vaccine to the two priority age groups. In addition, for the first time, a system updated weekly was used to estimate vaccination coverage in a large population of persons of all ages. These weekly reports were reviewed by KPNC to monitor compliance with ACIP guidelines. The cumulative KPNC results for the 2004--05 influenza season approximated those calculated nationally by the telephone-interview--based Behavioral Risk Factor Surveillance System (BRFSS) survey (5), although the two systems differ substantially. The KPNC estimates of vaccination coverage were calculated by using vaccinations recorded in the KPNC immunization registry and estimates of monthly enrollment of members in the northern California HMO. BRFSS estimates were based on the self-reported vaccinations of participating members of the civilian, noninstitutionalized population, regardless of health-insurance status, in all 50 states and the District of Columbia. In addition, the KPNC data include influenza vaccinations through April 2, 2005, whereas the BRFSS data include vaccinations through January 31, 2005. For adults aged >65 years, KPNC estimated coverage of 71.8%, and BRFSS estimated coverage of 62.7% (CI = 60.6%--64.8%). For adults aged 18--49 years, the estimates were 6.0% for KPNC and 6.9% (CI = 5.9%--7.9%) for BRFSS, and for adults aged 50--64 years, the estimates were 24.1% for KPNC and 16.5% (CI = 14.7%--18.3%) for BRFSS. Among children aged 6--23 months, KPNC estimated coverage of 57.4%, and BRFSS estimated coverage of 48.4% (CI = 39.6%--57.2%). Finally, for children aged 2--17 years, the estimates were 6.6% for KPNC and 12.3% (CI = 10.5%--14.1%) for BRFSS. According to both KPNC and BRFSS data, vaccine uptake was greatest in October and November and tapered off in December and January during the 2004--05 influenza season. The findings in this report are subject to at least four limitations. First, influenza vaccination coverage in an HMO might not be generalizable to the overall U.S. population. Second, estimates were obtained only from northern California; future assessments are expected to include additional HMOs in other regions. Third, enrollment figures from 2003 were used as a proxy for 2004--05 enrollment. Finally, certain KPNC members might have obtained influenza vaccinations outside of the HMO, resulting in an underestimate of vaccination coverage; however, such vaccination is unlikely because of the limited supply of influenza vaccine during the 2004--05 influenza season. Rapid analysis enabled weekly estimates of vaccination coverage in a KNPC population of 3.4 million. If expanded to all eight participating HMOs in the VSD, weekly vaccination coverage estimates could be provided for approximately 5.9 million HMO members (1.8% of the U.S. population). Unlike interview-based survey systems, the VSD vaccination data described in this report were not self-reported; they were collected from immunization registry data and therefore were not subject to recall bias. During the 2005--06 influenza season, the VSD rapid analysis system will perform its principal task of gathering data on potentially adverse events after vaccinations (e.g., with the new meningococcal conjugate vaccine [6]). However, the system also will be enhanced by additional HMO populations, and data on influenza vaccinees will enable weekly estimation of vaccination coverage among HMO members at high risk for influenza complications (3). References
* Group Health Cooperative (Seattle, Washington); Harvard Pilgrim Health Care, Harvard Medical, and Harvard Vanguard (Boston, Massachusetts); Health Partners Research Foundation (Minneapolis, Minnesota); Kaiser Permanente Colorado (Denver); Kaiser Permanente Northern California (Oakland); Kaiser Permanente Northwest (Portland, Oregon); Marshfield Clinic Research Foundation (Marshfield, Wisconsin); and UCLA Center for Vaccine Research/Southern California Kaiser Permanente Health Care Plan (Los Angeles).
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 7/13/2005 |
|||||||||
|