|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
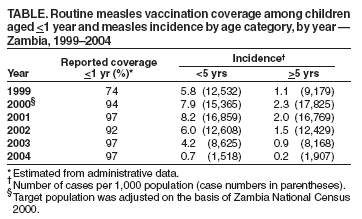
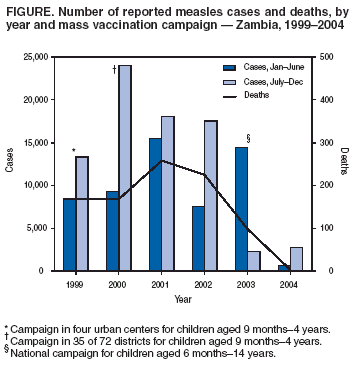
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress in Measles Control --- Zambia, 1999--2004Zambia, a southern African country with estimated population of 11.6 million in 2005 (1), reported 1,698--23,518 measles cases annually during 1991--1999. During that period, measles was considered one of the five major causes of morbidity and mortality among children aged <5 years (2). During 1999--2004, the challenge of controlling measles led Zambia to try several strategies in succession. In addition to a single dose of measles vaccine offered at age 9 months through routine services, in 1999, measles supplemental immunization activities (SIAs) targeting children aged 9 months--4 years were held in four urban centers. Those activities were followed in 2000 by a subnational measles SIA targeting children aged 9 months--4 years in approximately half of the country's 72 districts. In 2003, Zambia adopted a strategy of accelerated measles control that included strengthening routine vaccination, providing a second opportunity for measles immunization for all children, and conducting case-based surveillance. As part of this strategy, a nationwide measles SIA targeting all children aged 6 months--14 years was conducted in 2003. This report summarizes progress in measles control in Zambia during 1999--2004, as measured through surveillance data, which demonstrates a marked reduction in measles transmission after the 2003 SIA. Routine VaccinationThe routine vaccination program in Zambia provides a dose of measles vaccine to infants aged 9 months through fixed stations or through community outreach. The reported coverage with measles vaccine among children aged <1 year, as measured by the administrative method, was 74% in 1999 and 95% during 2000--2004 (Table). The administrative method for estimating vaccination coverage is calculated by dividing the reported number of vaccine doses administered by the number of children aged <1 year, as determined by the census and adjusted for annual growth; in Zambia, no adjustment is made for infant mortality. A 2002 cluster survey indicated routine 1-dose measles vaccine coverage of 84% among children aged <1 year. To further strengthen routine vaccinations, in January 2004, Zambia implemented the Reaching Every District (RED) strategy advocated by the World Health Organization (WHO) in the 10 districts with the highest number of unvaccinated children (3). Supplemental Immunization ActivitiesZambia conducted three measles SIAs during 1999--2003, which differed from each other in the age group targeted, geographic extent, and coverage achieved. The 1999 SIA targeted all children aged 9 months--4 years in the four urban districts of Kabwe, Kitwe, Lusaka, and Ndola, and achieved coverage of 81% as measured by the administrative method. The 2000 SIA focused on the eastern and northeastern border districts, targeted all children aged 9 months--4 years in 35 (49%) of the country's 72 districts, and achieved 91% coverage as measured by the administrative method. In June 2003, a nationwide SIA expanded the target population to all children aged 6 months--14 years and vaccinated 97% of the target population as measured by a vaccination coverage survey. This SIA also provided vitamin A supplementation and mebendazole anti-helminth treatment nationwide to children aged 6 months--4 years and insecticide-treated bed nets (ITNs) for malaria prevention and control to children in the same age group in one urban and four rural districts. SurveillanceMeasles is a notifiable disease in Zambia. The routine information system, including incidence and mortality data, was improved in 1998 with the addition of a nationwide district-based electronic system. Before July 2003, laboratory confirmation of cases was not performed routinely, and notifiable cases were those clinically suspected to be measles. Case-based measles surveillance with laboratory confirmation of each sporadic case or the first 5--10 outbreak cases was introduced after the 2003 SIA and is currently implemented nationwide. A national measles laboratory accredited by WHO provides routine enzyme-linked immunosorbent assay testing of serum specimens for measles IgM. During 1999--2003, an average of 26,072 suspected cases of measles were reported annually in Zambia, ranging from 16,793 cases in 2003 to 33,628 cases in 2001 (Figure). After the SIA in June 2003, an 87% decline occurred in the number of reported measles cases in the second half of 2003 (July--December), when compared with the average number of cases for the same period during the preceding 4 years (2,315 versus 18,220). The downward trend continued in 2004, during which 3,425 suspected cases were reported. Of these, 831 (27%) had a blood specimen submitted for confirmatory testing; of these 831 cases, 34 (4%) were positive for IgM antibody to measles. During 1999--2004, reported measles incidence by age group was threefold to fivefold higher among children aged <5 years, compared with persons aged >5 years (Table). Comparing the reported incidence before and after the June 2003 SIA (i.e., 2002 versus 2004), the declines were similar among children aged <5 years (88%) and persons aged >5 years (87%). During 1999--2002, the annual average number of deaths attributed to measles was 217, with an average of 110 deaths occurring during the first half of the year (January--June) and an average of 107 deaths occurring during the second half of the year. In 2003, a total of 86 measles deaths were reported during the first half of the year, and 12 deaths were reported during the second half. No measles deaths were reported during the first half of 2004; three deaths were reported during the second half of that year. Reported measles deaths declined by 99% in 2004 compared with the annual average reported during 1999--2002. Reported by: B Chirwa, V Mukonka, M Katepa, P Kalesha, Central Board of Health, Lusaka, Zambia. D Nshimirimana, A Onyeze, S Anyangwe, E Maganu, R Groves, World Health Organization. R Kezaala, KL Cairns, Global Measles Br, CDC. Editorial Note:A principal objective of the WHO Global Measles Strategic Plan for 2001--2005 is to decrease measles mortality by 50%, compared with 1999 levels, by 2005 (4). In addition, WHO has recommended that all children be provided a second opportunity for measles vaccination either through SIAs or routine health services (5). During 1999--2004, Zambia improved measles control by strengthening routine vaccination, providing a second opportunity for measles immunization through SIAs, and enhancing measles surveillance. Reported routine measles vaccine coverage increased >15% from 1999 to 2000, and has remained >90% in each of the preceding 5 years. This increase is attributable, in part, to 1) the twice-yearly Child Health Week immunization campaigns, which boosted routine vaccination by targeting unvaccinated children throughout the country, and 2) the drive to increase routine measles vaccination as a strategy to control measles epidemics. The reported increase in vaccination coverage might also be attributed, in part, to a change in population estimates. The 2000 census estimated approximately 10% fewer children aged <1 year compared with 1999 estimates, which had been projected from the 1990 census. Although the coverage survey conducted in 2002 suggests reported measles vaccination coverage might be an overestimate of true coverage, routine coverage likely has increased in recent years as a result of increased program activities. Zambia offered a second opportunity for measles vaccination through SIAs on three occasions during 1999--2004. However, measles morbidity and mortality declined substantially only after the most recent SIA in June 2003, which expanded the previous target population (i.e., children aged 9 months--4 years in selected geographic regions) to all children aged 6 months--14 years nationwide. This experience is similar to what has occurred in other African countries in the sub-Saharan region, where SIAs restricted to children aged <5 years or conducted subnationally resulted in transient decreases only in the targeted age groups and areas (2,6--8). The most likely explanations for this are: 1) subnational campaigns allow susceptible children to remain in geographic regions not targeted by SIAs, and population mixing then introduces these susceptible children to vaccinated regions, thus allowing virus transmission to persist; and 2) a substantial proportion of persons aged >5 years remain susceptible to measles, providing opportunity for ongoing transmission of virus both in this age group and to susceptible younger children. Approximately 50% of measles cases reported in Zambia during 1999--2003 occurred in children aged >5 years. Through the global initiative to eradicate poliomyelitis, Zambia has strengthened its vaccine delivery and surveillance systems and is now applying this capacity toward measles-control strategies. Case-based measles surveillance has been integrated with acute flaccid paralysis surveillance, and a reference laboratory has been established to provide confirmatory testing of serologic samples from suspected measles cases. The quality of measles case-based surveillance is monitored by two key indicators, the percentage of suspected measles cases with a blood specimen (24% in 2004; target: 80%) and the proportion of districts investigating at least one suspected measles case with a blood specimen per year (74% in 2004; target: 80%). Zambia achieved near-zero measles mortality and markedly reduced measles incidence after the 2003 national campaign. Routine vaccination and vaccine-preventable disease surveillance in Zambia is funded by the Zambian Ministry of Health and its partners (e.g., WHO, UNICEF, Government of Japan, and the Global Alliance for Vaccines and Immunization). The 2003 national measles SIA was funded by the Measles Partnership*. Bed net distribution was supported by the American Red Cross, the International Federation of Red Cross, and NETMARK, a malaria-related project of the Academy for Educational Development. To sustain these gains in measles control, Zambia must maintain high rates of routine measles vaccination (i.e., >90%), consider adding a second dose of measles vaccine to the routine vaccination schedule, work to sustain the quality of surveillance, and plan for a follow-up nationwide SIA to be held during 2006--2007. References
* In 2003, the Measles Partnership included the American Red Cross, the United Nations Foundation, WHO, UNICEF, Right to Play, and CDC.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 6/16/2005 |
|||||||||
|