|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
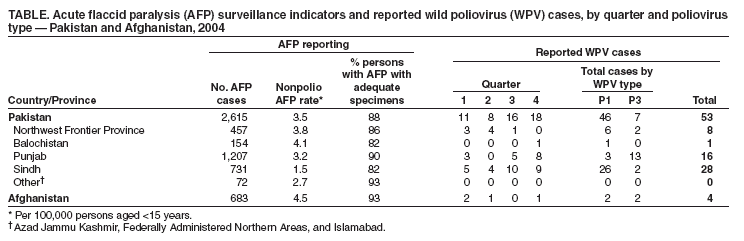
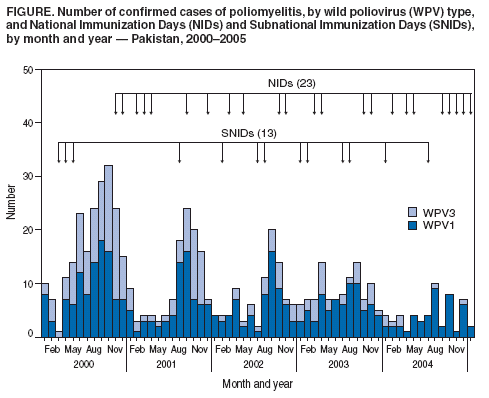
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- Afghanistan and Pakistan, January 2004--February 2005Although poliomyelitis remained endemic in only six countries at the end of 2003, a resurgence of polio occurred in 2004, originating in Nigeria and resulting in the export of wild poliovirus (WPV) into the polio-free countries of western and central Africa. However, progress toward interrupting WPV transmission continued during 2004 in Afghanistan, India, and Pakistan, the only remaining countries in Asia where polio is endemic (1,2). This report summarizes progress toward polio eradication in Afghanistan and Pakistan during January 2004--February 2005 and indicates that, with continued support from national and local leaders, interruption of poliovirus transmission in both countries is feasible by the end of 2005. Immunization ActivitiesRoutine infant vaccination coverage with oral poliovirus vaccine (OPV) remains low in Afghanistan and in multiple areas of Pakistan (2). To increase population immunity, both countries continued in 2004 to provide children aged <5 years with additional OPV doses during large-scale, house-to-house supplementary immunization activities (SIAs), conducted approximately every 6 to 8 weeks. Closely synchronized between the two countries, eight SIA rounds were conducted in 2004 (Figure), and two rounds (mid-January and early March) have already been conducted in 2005. All rounds were nationwide, except for the December 2004 and January 2005 rounds in Afghanistan, which targeted approximately 60% of children aged <5 years in selected provinces, and the June round in Pakistan, which also targeted approximately 60% of children aged <5 years. In both countries, activities to improve the effectiveness of SIAs focused on two areas: 1) advocacy with political, religious, and health leaders and 2) continued improvement of managerial and supervisory processes. Advocacy at national, provincial, and district levels was crucial to maintaining and improving leaders' commitment and support for polio eradication. National Ministry of Health (MOH), World Health Organization (WHO), and United Nations Children's Fund (UNICEF) polio teams further improved SIA effectiveness by continuing to monitor activities and by providing additional technical support for regions with remaining virus transmission and for other areas with performance problems during SIAs (e.g., security-compromised areas with difficult access or culturally conservative areas where access to homes is limited). Acute Flaccid Paralysis (AFP) SurveillanceAFP surveillance has remained sensitive and has improved overall in both Afghanistan and Pakistan. Surveillance quality is measured by two primary indicators: 1) the nonpolio AFP rate (at least one nonpolio AFP case per 100,000 persons aged <15 years) and 2) the completeness and timeliness of stool-specimen collection (at least 80% of AFP cases with two adequate stool specimens collected from patients within 14 days of paralysis onset). Both indicators were at target values or higher in 2004 in both Afghanistan and Pakistan at the national and provincial levels. In Pakistan, targets were also reached in 80% of districts; 24 of 121 districts in Pakistan failed to reach the target of collecting adequate stool specimens in 80% of reported cases. Pakistan conducted detailed provincial reviews of AFP surveillance quality during the fourth quarter of 2004 in Balochistan and Northwest Frontier Province (NWFP), where no WPV was isolated for prolonged periods (15 months in Balochistan and 4 months in NWFP). The two provinces meet the surveillance quality indicator targets, with some need for improvement in active surveillance, particularly in NWFP. To increase the overall sensitivity of the surveillance system, the sampling of direct contacts of AFP patients was expanded to include the contacts of 1) any child for whom stool-specimen collection was inadequate or 2) patients for whom the adequacy of specimen storage and shipment was in doubt. As a result, in 2004, WPV was isolated from direct contacts of two virus-negative AFP patients. Surveillance teams were trained with new guidelines to reduce the inappropriate exclusion of AFP cases, resulting in an observed increase in overall AFP reporting during the second half of 2004. However, genetic sequencing* of viruses indicates that some virus lineages continued to circulate at low levels for at least 1.5 years without being detected, suggesting that gaps in surveillance sensitivity likely persist in certain areas, particularly in southern Punjab and Sindh provinces. Afghanistan achieved high nonpolio AFP rates of at least 2.0 per 100,000 population, with collection of adequate specimens from >80% of AFP patients in all regions in 2004. Nonpolio AFP rates and adequate stool specimen collection were lowest in the southern and southeastern regions. In those areas, continued security problems impaired surveillance; genetic data suggest that the wild poliovirus type 3 (WPV3) detected in December 2004 in the southern region had been circulating undetected for more than 1 year. Incidence of PolioFrom 2003 to 2004, the number of reported polio cases decreased approximately 50% in both countries, from 103 to 53 cases in Pakistan (46 wild poliovirus type 1 [WPV1] and seven WPV3) and from eight to four cases (two WPV1 and two WPV3) in Afghanistan. Polio continued to affect the very young, with 68% of cases (36 of 53) in Pakistan and two of four cases in Afghanistan in the <24-month age group. Vaccination status of cases was reported as >3 doses of OPV received for 36 cases (68%) in Pakistan and three of four cases in Afghanistan. WPV1 has not been identified for nearly 1 year in Afghanistan, the longest period without detection since the introduction of AFP surveillance in 1997. Two WPV1 isolates detected in early 2004 in the security-affected southern region belonged to the same WPV1 lineage cluster identified later in the year in northern Sindh and southern Punjab provinces of Pakistan. WPV3 detected in May 2004 in Jalalabad, eastern region, and in late December near Kandahar, southern region, belong to WPV3 lineage clusters discovered in both countries in 2004; genetic sequence data indicate that the December 2004 WPV3 lineage circulated undetected for more than 1 year. In 2004, two Pakistan provinces, Balochistan and NWFP, experienced long polio-free intervals (Table). In Balochistan, WPV was not detected for 15 months, from October 2003 to December 2004, when WPV1 (genomic sequencing pending) was detected in southeastern Balochistan, adjacent to a district of northern Sindh in which WPV is endemic. In 2004, WPV was not detected in NWFP from September through December, historically the peak transmission season. A WPV1 case was identified in early August with close genetic relation to a WPV1 lineage cluster cocirculating in Sindh. In January 2005, a WPV1 was isolated in Peshawar, NWFP, that was genetically related to other NWFP polioviruses. Punjab, Pakistan's most densely populated province, reported three cases during the first half of 2004 and 14 cases, primarily from southern Punjab, during the second half. Genetic sequencing suggests that certain viruses identified in Punjab were directly imported from NWFP and Sindh. However, sequence analysis also reveals that at least two WPV1 and one WPV3 lineage detected in Punjab in 2004 are at least 1.5% different from their nearest genetic neighbor. This indicates the lineages must have circulated without detection by AFP surveillance for approximately 1.5 years or more based on the mutation rate of the genetic segment being sequenced. In 2004, Sindh became the most consistently polio-endemic province. Virus circulation in Sindh in 2004 occurred primarily in the north of the province in the first half of the year and in south-central Sindh in the second half. Sporadic transmission has continued in early 2005 in both southern Punjab (two WPV1 cases) and Sindh (two WPV1 cases). Reported by: Immunization, Vaccines, and Biologicals Dept, World Health Organization (WHO), Geneva, Switzerland. WHO Pakistan, Islamabad. Global Immunization Div, National Immunization Program, CDC. Editorial Note:Afghanistan and Pakistan progressed further toward polio eradication in 2004. Both countries reported 50% fewer cases in 2004, compared with 2003. In addition, WPV was not reported for 15- and 4-month intervals in Balochistan and NWFP, respectively, even though sensitive surveillance was maintained. Faced with the continued challenge of preparing, implementing, and evaluating large, nationwide immunization rounds, both countries managed to maintain and improve SIA quality. SIA monitoring is used to identify low-performing areas rapidly and to rectify problems during the round or before the next round. However, serious challenges remain. Continued WPV transmission in parts of both countries, particularly in Sindh and Punjab in Pakistan and in the southern region of Afghanistan, indicates that SIAs still do not produce levels of population immunity required for interrupting the remaining chains of transmission. Although SIA quality is improving, children are still being missed. To address this problem, national and local governments are urged to increase their commitment to the global polio eradication program. Support of the program by national and local leaders is one of the strongest determinants of SIA quality. In addition, specific steps have been taken to increase access to children. These include increasing access to homes in which no male family member is present by increasing the proportion of vaccination team members who are women and negotiating access to homes in culturally conservative areas. Measures have also been taken to improve the quality and efficiency of vaccination team supervision. These measures include increased training of field supervisors and increased numbers of WHO district support staff members assigned to expand interventional monitoring in difficult and low-performing districts. AFP surveillance in both Afghanistan and Pakistan meets or exceeds WHO performance-indicator targets in most areas and is continuously reviewed to detect quality gaps and respond to them quickly. As transmission of poliovirus decreases overall, finding the remaining sources of transmission becomes even more challenging. Reliable detection of virus will require further increase in the overall sensitivity of the surveillance system and detailed epidemiologic information. Viruses that are genetically distant from their nearest phylogenetic neighbor have been identified in high-risk areas of both countries. The absence of more closely related viruses indicates that lineages are circulating undetected and AFP surveillance might still be missing cases. To date, the achievements toward eradicating polio in Afghanistan and Pakistan would not have been possible without continued financial and technical support from the international polio partnership, especially from political and health leaders at national, provincial, and district levels in both countries. Available evidence indicates that, with continued support, interruption of WPV transmission in both countries can be accomplished by the end of 2005. References
* The genetic sequence of the complete VP1 coding region is determined by using automated dye-labeled cycle sequencing procedures described previously (3) and the resulting sequences compared to a database of all recent poliovirus isolates. The comparisons are summarized through phylogenetic analysis.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 3/24/2005 |
|||||||||
This page last reviewed 3/24/2005
|