|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
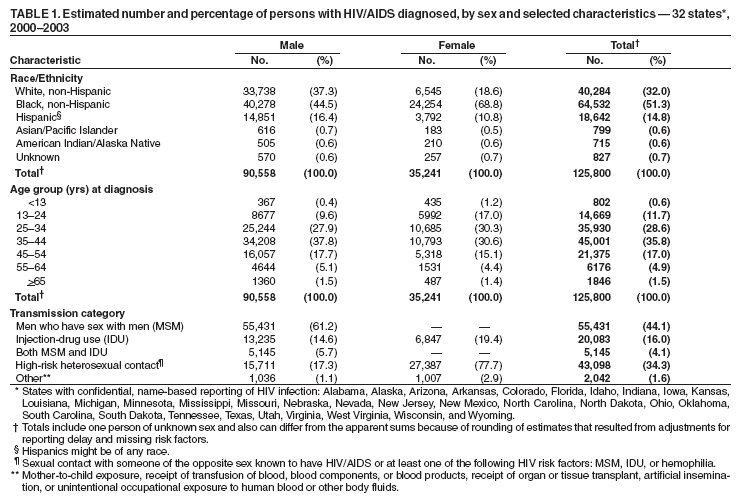
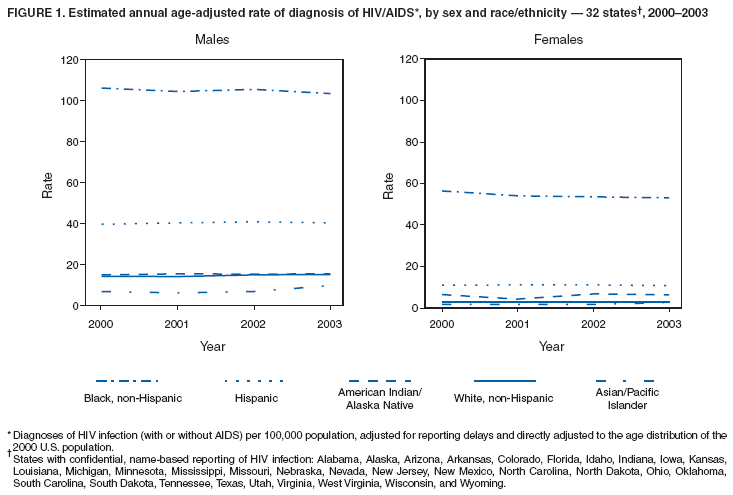
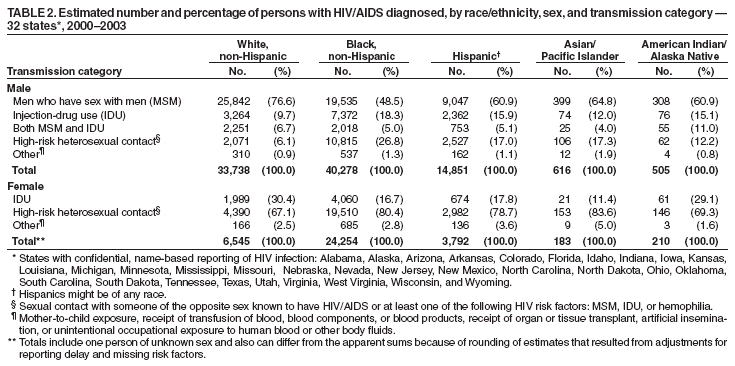
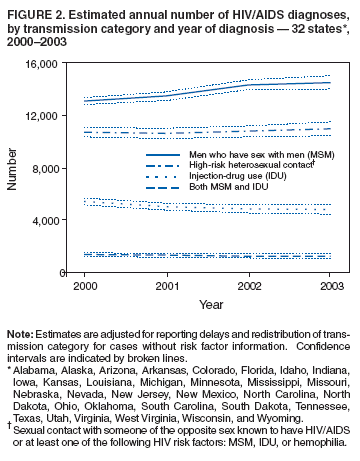
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Diagnoses of HIV/AIDS --- 32 States, 2000--2003An estimated 850,000--950,000 persons in the United States are living with human immunodeficiency virus (HIV), including 180,000--280,000 who do not know they are infected (1). To examine trends of diagnoses for 2000--2003, CDC analyzed HIV and acquired immunodeficiency syndrome (AIDS) together as HIV/AIDS (i.e., HIV infection with or without AIDS), counted by the year of earliest reported diagnosis of HIV infection. From 2000 to 2003, in 32 states* that used confidential, name-based reporting of HIV and AIDS cases for >4 years, the overall annual rate of diagnosis of HIV/AIDS remained stable. However, rates among non-Hispanic black females were 19 times higher than rates among non-Hispanic white females, underscoring the need for continued emphasis on programs targeting females in racial/ethnic minority populations to reduce the number of cases of HIV/AIDS. CDC surveillance reports of HIV/AIDS are limited to cases among residents of states and U.S. territories where surveillance for non-AIDS HIV infection is conducted by using the same confidential, name-based reporting approach as for AIDS case reporting (2). The number of states conducting HIV/AIDS surveillance in this manner has gradually increased, resulting in available data for a greater proportion of cases in the United States. Numbers of cases, age-adjusted rates, and associated confidence intervals (CIs) were calculated, adjusting for random variation, reporting delay, and missing information on HIV risk factors (e.g., men who have sex with men [MSM] and injection-drug use [IDU]) (3,4). Data from territories were not included in this analysis. Cases were classified in the following hierarchy of transmission categories: MSM, IDU, both MSM and IDU, high-risk heterosexual contact (i.e., with someone of the opposite sex known to have HIV/AIDS or a risk factor [e.g., MSM or IDU] for HIV/AIDS), and all other HIV risk factors combined. Age-adjusted rates were calculated by the direct method, using the age distribution of the 2000 U.S. population as the standard. The statistical significance of differences between a pair of rates was assessed by the z test. To estimate the annual proportional change in a rate or number of diagnoses during 2000--2003, the logarithm of the rate or number was fit to a linear model. The significance of a trend was assessed by determining whether the 95% CI for the estimated annual proportional change included zero. During 2000--2003, HIV/AIDS was diagnosed in 125,800 persons who resided in the 32 states. Of these persons, 35,241 (28.0%) were female (Table 1). Although non-Hispanic blacks constituted 13% of the population of the 32 states during these 4 years (5), they accounted for more than half (64,532 [51.3%]) of the HIV/AIDS diagnoses, including 68.8% of diagnoses among females and 44.5% of those among males. The remaining cases were among non-Hispanic whites (40,284 [32.0%]), Hispanics (18,642 [14.8%]), Asians/Pacific Islanders (799 [0.6%]), and American Indians/Alaska Natives (715 [0.6%]). Non-Hispanic blacks constituted 35.2% of cases in the MSM transmission category, 56.9% of cases in the IDU transmission category, 70.4% of cases in the high-risk heterosexual contact category, and 69.8% of cases of mother-to-child transmission. The transmission category with the largest proportion of males with HIV/AIDS was MSM (61.2%), followed by high-risk heterosexual contact (17.3%), and IDU (14.6%) (Table 1). The transmission category with the largest proportion of females with HIV/AIDS was high-risk heterosexual contact (77.7%), followed by IDU (19.4%). The proportional distribution of cases by transmission category varied by race/ethnicity (Table 2). During 2000--2003, annual age-adjusted rates of HIV/AIDS diagnosis per 100,000 population changed little (Figure 1). Overall, the rate increased 1.0%, from 19.5 in 2000 to 19.7 in 2003. Further analyses indicated statistically significant (p<0.05) changes among certain populations. The rate among males increased 3.0% (from 27.9 to 28.8), and the rate among females decreased 3.7% (from 11.2 to 10.8). The rate among non-Hispanic white males increased 6.2% (from 14.3 to 15.2), and the rate among Asian/Pacific Islander males increased 39.7% (from 7.0 to 9.8); the rate among non-Hispanic black females decreased 6.0% (from 56.4 to 53.0). Trends in annual age-adjusted rates among other sex and racial/ethnic groups were not significant. Rates among non-Hispanic black females were 19 times the rate among non-Hispanic white females, five times the rate among Hispanic females, and also higher than rates among males in any racial/ethnic population other than non-Hispanic blacks. Rates among non-Hispanic black males were seven times higher than those among non-Hispanic white males and three times higher than those among Hispanic males. Statistically significant trends in the annual number of diagnoses included a 4.9% increase, from 2000 to 2003, among males (from 22,117 to 23,203). A 2.1% decrease among females (from 8,986 to 8,791) was not statistically significant. The increasing rate and number of diagnoses among males largely reflected the upward trend in the number of diagnoses associated with MSM, which increased 10.8% (Figure 2) from 13,099 to 14,510, consistent with the trend previously reported (6). The number of diagnoses associated with the combination of MSM and IDU decreased 10.3% (from 1,363 to 1,223). Reported by: RM Selik, MD, MK Glynn, DVM, MT McKenna, MD, Div of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:The analysis of surveillance data for 2000--2003 reveals overall stable annual rates of HIV/AIDS diagnosis; these rates reflect the interaction between HIV incidence and HIV testing. CDC has determined that national HIV incidence has been stable since the early 1990s (7) and that 25% of those living with HIV do not know they are infected (1). The stable rates during 2000--2003 suggest that enhanced prevention efforts are needed to decrease HIV incidence and increase knowledge of HIV status. In 2003, CDC launched Advancing HIV Prevention (AHP), an initiative aimed at reducing barriers to early diagnosis of HIV and increasing access to quality medical care, treatment, and ongoing prevention services for HIV-infected persons (8). The availability of simple, rapid HIV tests, including those that use oral fluid, should increase testing opportunities for those at high risk for HIV; rapid testing was first implemented in U.S. prevention programs in late 2003. As part of AHP, CDC also encourages physicians to routinely provide prevention messages and screening for sexually transmitted diseases for their patients who are HIV positive (9). For those persons who have difficulty initiating and sustaining safer behaviors, more intensive interventions (e.g., individualized support and counseling through prevention case management or multisession behavioral interventions) might be beneficial. Rates among non-Hispanic blacks, and to a lesser extent Hispanics, are substantially greater than rates among non-Hispanic whites in the United States. Race/ethnicity likely is associated with behavioral risk factors and underlying socioeconomic circumstances and barriers to risk reduction. To eliminate racial/ethnic disparities, opportunities for early diagnosis of HIV infection should be expanded. In addition, culturally sensitive prevention programs should be improved to promote avoidance of risk factors (e.g., by having only one sex partner of known infection status or abstaining from sex and illicit drug use) and to reduce the harm from risk factors (e.g., by using condoms correctly and consistently and by using aseptic practices to prevent transmission from IDU). The findings in this report are subject to at least one limitation. Confidential, name-based HIV/AIDS surveillance was not conducted in all states and territories. The 32 states included in the analysis accounted for only 49% of the national total of AIDS diagnoses (excluding U.S. territories) during the same period and might not be nationally representative. Data from states with the highest AIDS morbidity in 2003 (e.g., California and New York) were not included. However, on the basis of national AIDS statistics with similar patterns, the racial/ethnic disparities in HIV/AIDS described in this report likely are indicative of substantial disparities nationwide (10). In 2003, CDC reported a 17% increase in HIV/AIDS diagnoses in MSM, from 1999 to 2002, in 29 states; the largest increase occurred from 2001 to 2002. For this report, an 11% increase was observed in HIV/AIDS diagnoses in MSM from 2000 to 2003 in 32 states, with the largest increase occurring from 2001 to 2002. MSM continue to constitute a substantial proportion of HIV/AIDS cases. CDC funds prevention programs for MSM, including counseling and testing through community outreach. Effective behavioral interventions for MSM include conducting small group sessions on HIV transmission, training in how to negotiate risk reduction, such as condom use, and training of popular opinion leaders in how to promote risk reduction or elimination. CDC also funds prevention activities for females that emphasize 1) better integration of testing, treatment, and prevention services for all females; 2) recognition of the relationship between drug use and sexual transmission of HIV; 3) research on effective female-controlled prevention methods for women unwilling or unable to negotiate condom use with a male partner; 4) and programs proven effective for changing risky behavior and sustaining those changes over time. CDC funds 104 community-based organizations involved in HIV/AIDS prevention, for which >15% of the target populations are females; 84% of these groups serve black females and 72% Hispanic females. Most of these prevention activities are funded through the Minority AIDS Initiative, a capacity-building initiative that supports implementation of effective prevention interventions among racial/ethnic minority populations. A sustained, comprehensive effort is required to reduce racial/ethnic disparities in HIV/AIDS diagnoses among females. References
* Alabama, Alaska, Arizona, Arkansas, Colorado, Florida, Idaho, Indiana, Iowa, Kansas, Louisiana, Michigan, Minnesota, Mississippi, Missouri, Nebraska, Nevada, New Jersey, New Mexico, North Carolina, North Dakota, Ohio, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, West Virginia, Wisconsin, and Wyoming.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 12/1/2004 |
|||||||||
This page last reviewed 12/1/2004
|