|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
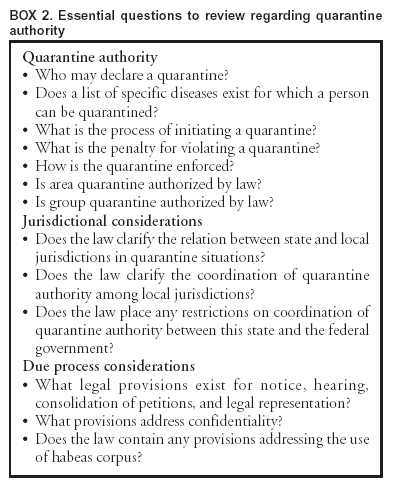
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Postexposure Prophylaxis, Isolation, and Quarantine To Control an Import-Associated Measles Outbreak --- Iowa, 2004On March 12, 2004, a college student infectious with measles returned to Iowa from India by a commercial airliner (1); the case was subsequently linked to two other measles cases. This report updates information about this outbreak and provides details regarding vaccination, quarantine, and other measures used by Iowa public health authorities to interrupt disease transmission in a vulnerable population. The effective uses of quarantine and isolation during the outbreak underscore the utility of these public health tools in halting communicable disease transmission. Immediately after being notified of the measles case, the Iowa Department of Public Health (IDPH) and local health departments in Iowa began using media releases, passenger lists, and interviews with the infected student to identify and contact persons potentially exposed to measles. Susceptible contacts (i.e., persons exposed and not fully vaccinated) were offered postexposure prophylaxis (PEP), either measles-mumps-rubella (MMR) vaccination within 72 hours of exposure or immune globulin (IG) within 6 days of exposure. Approximately 10 days later, measles cases were identified in two other Iowa residents: 1) a fellow airline passenger who previously had received two MMR vaccinations and 2) an unvaccinated close contact who had received postexposure MMR vaccination approximately 26 hours after contact with the first patient. Contacts of these two patients also were identified and offered PEP if they were deemed susceptible to measles infection. In public health immunization clinics specifically organized to vaccinate persons who had been exposed to measles, approximately 175 persons received postexposure MMR vaccination, and 20 received postexposure IG. All three patients, who were moderately ill, were placed in voluntary isolation, which IDPH and local health departments monitored with home visits and telephone calls. Two susceptible health-care workers, who were exposed when the second patient sought medical care and who did not receive PEP within the recommended period, were placed in voluntary quarantine for 2 weeks, during which they did not leave their homes. Two of the three measles patients were part of an insular community (estimated population: 2,000--3,000) with low vaccination rates (i.e., the community's K--12 school had a vaccination rate of 59% for vaccines required for school entry, including MMR). Community members held daily gatherings that provided opportunities for measles transmission to susceptible persons. PEP was offered to all susceptible persons in the community, and 56 accepted. Seven persons who had potentially been exposed to measles refused PEP, even though they were aware of the potential for being quarantined. Initially, all seven agreed to be quarantined in lieu of receiving vaccine, but because of their subsequent unwillingness to comply with voluntary quarantine, all seven were served by the local public health nurse with state-issued involuntary home quarantine orders, some with the assistance of local law enforcement officers. (Examples of Iowa's quarantine orders are available at http://www.idph.state.ia.us/adper/cade.asp.) Although none reported a history of full vaccination or symptomatic measles, within days of being quarantined, four of the seven were determined serologically to be immune and were released from quarantine; the other three completed their 2-week quarantine. IDPH and the local health department monitored compliance with quarantine orders with at least daily unannounced home visits or telephone calls and released the persons from quarantine via oral communication. In the future, because of confusion about the exact time of day the quarantine should end, written release-from-quarantine notices will be served. No known breaks in quarantine occurred. None of those persons in quarantine acquired measles. No additional cases were reported. Reported by: V McKeever, Jefferson County Public Health, Iowa; H Adams, JD, Office of the Iowa Attorney General; T Thornton, P Quinlisk, MD, Iowa Dept of Public Health. M Cetron, MD, Div of Global Migration and Quarantine, National Center for Infectious Diseases; R Goodman, MD, JD, F Shaw, MD, JD, A Moulton, PhD, Public Health Law Program, Office of the Chief of Public Health Practice; M Papania, MD, National Immunization Program, CDC. Editorial Note:Use of vaccination, both pre- and postexposure, is the most common and preferred strategy for preventing transmission of measles (2). During this outbreak, Iowa public health officials first offered timely postexposure vaccination to susceptible persons who had close contact with a person infected with measles. However, when postexposure vaccination was refused, quarantine was used to reduce the risk of further transmission of measles to a vulnerable population. An essential public health tool, rarely used in the last half century in the United States, quarantine is often confused with isolation, which is the restriction of movement of persons who are known to be infected with a communicable disease and who often are symptomatic. Quarantine reduces the risk of exposure to disease by separating and restricting the movement of persons who are not yet ill but who have been exposed to an infectious agent and might become infectious. Quarantine is more difficult to implement than isolation because the persons under quarantine are not symptomatic and thus have greater difficulty understanding the need for staying at home when compared with ill persons who need to be isolated. Before antibiotics and vaccines, quarantine was used when direct medical countermeasures were not routinely available. However, quarantine often was implemented in a manner that equated disease with crime; consequently, quarantine acquired negative connotations associated with stigma and discrimination. For quarantine to be an effective and acceptable public health tool, these negative connotations must be overcome by applying the measure equally and fairly among all persons who have been exposed, and by using other approaches. These include providing education about the rationale for using quarantine; offering acceptable alternatives to quarantine, when feasible, such as postexposure vaccination or obtaining serologic proof of immunity; and applying due process measures, such as written notice and opportunities to appeal. The use of quarantine to address public health problems demands a balancing of individual civil liberties with the collective needs of the public's health. Additional focus on the health, welfare, and social needs of persons subjected to quarantine is required. During the 2003 epidemic of severe acute respiratory syndrome (SARS), CDC listed 10 principles for modern quarantine (Box 1) (3,4). In the United States, as in most countries of the world, government has the duty and legal power to address risks associated with persons whose freedom of movement might endanger the public's health. Under circumstances described in federal statute*, the U.S. government has the authority to detain persons for the control of communicable diseases. In particular, the U.S. government has the authority to isolate and quarantine persons to control the spread of selected communicable diseases specified by presidential executive order (5,6). In addition, all 50 states and the District of Columbia have the authority to detain persons under their own quarantine laws. In the event of an epidemic resulting from natural transmission or from deliberate introduction, both state and federal quarantine laws could be invoked to stem the spread of disease. After the events of September 11, 2001, and in response to the draft Model State Emergency Health Powers Act (7), Iowa lawmakers reviewed the state's legal authority for public health emergency preparedness and response. In 2003, as a result of this review, the Iowa state legislature enacted new laws related to public health disaster preparedness. The new legislation included a provision authorizing IDPH to order quarantine in the event of a public health disaster†. To implement this legislation and preexisting laws authorizing quarantine in nondisaster situations, IDPH adopted administrative rules governing the quarantine process. These rules became effective on March 10, 2004, only 2 days before the measles-infected student returned home to Iowa. Although the measles outbreak did not constitute a public health disaster under the 2003 statute, the state used the new quarantine process as outlined in its administrative rules to assist in containing the outbreak. In 2003, the SARS outbreak triggered the widest use of quarantine globally since the influenza pandemic of 1917. Largely voluntary quarantine was used in Canada to keep approximately 20,000 persons in their homes for 10 days (8). For 27 persons who refused voluntary quarantine, public health officials issued legally enforceable quarantine orders. In certain cities in Asia (e.g., Beijing, Hong Kong, Singapore, and Taipei), quarantine authority was used to order thousands of persons to remain in their homes, an intervention that has been credited with helping to contain the outbreak (3). Although SARS did not spread within the United States, certain jurisdictions used quarantine authority to minimize the risk of spreading the virus (e.g., via unprotected health-care workers exposed to infectious SARS patients). The scope and specifics of laws authorizing quarantine vary substantially by state. States that have not reviewed their quarantine laws might consider doing so by using a systematic approach covering essential features (e.g., quarantine, jurisdictional aspects, and due process) (Box 2). State and local health officials also might consider reviewing quarantine-related laws with their agencies' legal counsels, in coordination with law enforcement officials and the judiciary. References
* 42 U.S.C. § 264. † Iowa Code section 135.144 (2003 Suppl.), 139A.4, 139A.9, and 641 Iowa Administrative Code chapter 1.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/21/2004 |
|||||||||
This page last reviewed 10/21/2004
|