|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
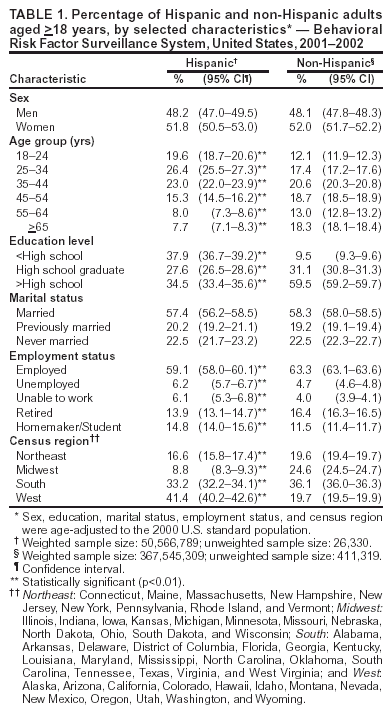
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Access to Health-Care and Preventive Services Among Hispanics and Non-Hispanics --- United States, 2001--2002Although Hispanics are the largest ethnic minority population in the United States, they are underserved by the health-care system (1). Hispanics are less likely to seek and receive health-care services, which might contribute to their poorer health status and higher rates of morbidity and mortality (2). To assess differences in access to health-care and preventive services between Hispanics and non-Hispanics, CDC analyzed 2001--2002 data from the Behavioral Risk Factor Surveillance System (BRFSS) surveys. This report summarizes the results of that analysis, which indicated that disparities exist in access to health-care and preventive services among Hispanics versus non-Hispanics. Public health authorities and health-care providers should implement strategies to reduce barriers to health-care and preventive services among Hispanics. BRFSS is a state-based, random-digit--dialed telephone survey of the U.S. civilian, noninstitutionalized population aged >18 years. All 50 states and the District of Columbia participated in the surveys for 2001--2002, the latest years for which data were available. Respondents with complete information on age, race/ethnicity, education, sex, marital status, and employment status were included. Analyses were adjusted for respondents' sex, marital status (i.e., married, previously married, or never married), employment status (i.e., employed, unemployed, unable to work, retired, or homemaker/student), and self-rated general health status to control for potential confounders. Respondents' receipt of selected preventive services and access to health care were assessed. Clinical preventive services included mammography within 2 years among women aged >40 years, cervical cancer screening within 3 years among women with an intact uterus (i.e., no hysterectomy), fecal occult blood testing within 2 years among adults aged >50 years, sigmoidoscopy/colonoscopy within 5 years among adults aged >50 years, blood cholesterol checked within 5 years among adults aged >18 years, influenza vaccination within the previous year among adults aged >65 years, and pneumococcal vaccination among adults aged >65 years. Data on breast and cervical cancer and medical care were collected in 2002, data on blood cholesterol were collected in 2001, and data on colorectal cancer screening, vaccination, and health-care coverage were collected in 2001 and 2002. Interviews were conducted in English and in Spanish when applicable. Health-care coverage was assessed by asking respondents, "Do you have any kind of health-care coverage, including health insurance, prepaid plans such as HMOs, or government plans such as Medicare?" Having a regular care provider was assessed by asking, "Do you have one person you think of as your personal doctor or health-care provider?" Persons who responded "no" were asked, "Is there more than one or is there no person who you think of?" To be classified as having a regular care provider, respondents must have responded either "yes, only one" or "more than one." Inaccessibility to medical care at some point during the preceding 12 months was assessed by asking, "Was there a time in the past 12 months when you needed medical care, but could not get it?" Having a regular place of care was assessed by asking, "When you are sick or need advice about your health, to which one of the following places do you usually go? Would you say: a doctor's office, a public health clinic or community health center, a hospital outpatient department, a hospital emergency room, urgent care center, some other kind of place, or no usual place?" For this analysis, having a regular place of care was dichotomized into 1) a doctor's office, public health clinic or community health center, hospital outpatient department, hospital emergency room, urgent care center, or some other kind of place and 2) no usual place. The BRFSS data files were edited and aggregated to create a yearly sample for each state. Each sample was weighted to the respondent's probability of selection and to age- and sex-specific or race-age and sex-specific population from the most current census data. To compare Hispanics and non-Hispanics, prevalence estimates were adjusted to the 2000 U.S. standard population. SUDAAN® (Research Triangle Park, North Carolina) was used to account for the complex sampling design and to calculate the standard errors and 95% confidence intervals (CIs). All results were statistically significant (p<0.01 or p<0.05) unless otherwise noted. In 2002, a total of 247,964 interviews were completed; 18,152 (7.3%) were by Hispanic respondents, and 229,812 (92.6%) were by non-Hispanic respondents. The median response rate was 58.3% (range: 42.2%--82.6%). In 2001, a total of 212,510 interviews were completed; 17,588 (8.3%) were by Hispanic respondents, and 194,922 (91.7%) were by non-Hispanic respondents. The median response rate was 51.1% (range: 33.3%--81.5%). Hispanic respondents were significantly more likely than non-Hispanic respondents to be aged 18--44 years; have less than a high school education; be unemployed, unable to work, or a homemaker or student; reside in Western states*; and report fair or poor general health (Tables 1 and 2). Hispanic respondents were significantly less likely than non-Hispanic respondents to have health-care coverage (76.2% versus 90.6%), have one or more regular personal health-care providers (68.5% versus 84.1%), or have a regular place of care (93.4% versus 96.2%) (Table 2). Hispanic respondents were significantly more likely than non-Hispanic respondents to report having needed medical care during the preceding 12 months but could not obtain it (6.5% versus 5.0%). Hispanics also were significantly less likely to be screened for blood cholesterol and for breast, cervical, and colorectal cancers; to receive a pneumococcal vaccination; and to receive an influenza vaccination within the preceding year. Reported by: LS Balluz, ScD, CA Okoro, MS, TW Strine, MPH, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Disparities in use of preventive services by racial/ethnic characteristics have been documented (3); minority populations, such as Hispanics, are less likely than non-Hispanics to receive preventive services (3). This report demonstrates that these disparities in access to health-care and screening practices between Hispanics and non-Hispanics persist. Substantial differences in prevalence of health-care coverage (i.e., having a regular personal health-care provider or a regular doctor among those with a regular place of care) were documented among Hispanics compared with non-Hispanics. These differences remained significant even after adjusting for respondents' socioeconomic factors and self-rated health status. In the United States, access to health care is closely related to insurance coverage, the type of insurance, and whether persons have a regular source of care (4). Having access to health care increases the use of preventive services (4). The lower prevalence of health-care access among Hispanics might explain the disparities in receiving preventive services. Hispanic adults were substantially less likely than non-Hispanic adults to receive cancer screenings, blood cholesterol screening, or recommended vaccinations. Hispanics face obstacles in accessing health-care services in the United States, such as cultural differences between them and their health-care providers, language barriers, and the administrative complexity of health plans. Such obstacles might place Hispanics at increased risk for not seeking preventive services and for poor quality of care (5,6). Cultural factors also might affect Hispanics' access to preventive services. Hispanics have less knowledge about cancer and a more fatalistic attitude toward cancer than non-Hispanics (7,8). Cancer is increasing among Hispanics (9), and cancer screening, an essential component of early detection and treatment, is especially important among Hispanics. The findings in this report are subject to at least three limitations. First, data were based on self report and subject to recall bias. Second, BRFSS is a telephone survey; therefore, persons without telephones were not surveyed. Third, states that conducted the survey only in English excluded persons who speak only Spanish. Strategies to reduce barriers to health-care and preventive services should be developed among Hispanics. These include using culturally appropriate programs to advise Hispanics about the importance of screening, expanding access to health care, and targeting specific barriers to care, such as poverty and lack of knowledge among health-care professionals about how best to encourage Hispanics to use preventive services. References
* Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. Table 1Table 2
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/14/2004 |
|||||||||
This page last reviewed 10/14/2004
|