 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tuberculosis Transmission in a Renal Dialysis Center --- Nevada, 2003Among persons with chronic renal failure, infection with Mycobacterium tuberculosis is more likely to progress to tuberculosis (TB) (1,2). Chronic renal failure is an immunocompromising condition associated with cutaneous anergy, which can result in a false-negative tuberculin skin test (TST) result (3--5). In 2003, a health-care worker (HCW) (i.e., a hemodialysis technician) in an outpatient renal dialysis center in Nevada became ill with pulmonary TB, exposing more than 400 patients and other employees. The HCW had a previous positive TST result but never received treatment for TB infection. This report summarizes the results of a contact investigation, which suggested that the HCW had transmitted M. tuberculosis to 29 patients and 13 employees. The findings underscore the need for TB screening and treatment of TB infection for all HCWs and patients at high risk. Before diagnosis in August 2003, the HCW had experienced 6 weeks of cough, fatigue, and a 14-pound weight loss. Microscopic examination of sputum was 4+ positive for acid-fast bacilli (AFB), indicating infectiousness, and sputum culture yielded M. tuberculosis susceptible to all first-line anti-TB medications. The HCW was considered infectious for 3 months before TB diagnosis. During the 3-month period, employees and patients in the dialysis center were considered contacts and evaluated. Employee work schedules and patient dialysis schedules were reviewed to quantify the cumulative hours each person had been exposed to the HCW. In September 2003, initial screening of exposed persons included review of medical history, TB symptoms, and previous TST results. Persons without a previous positive TST result received a TST. All dialysis patients were referred for chest radiographs. Persons with TB symptoms or an abnormal chest radiograph submitted sputum for AFB testing and culture. Persons with a negative TST result (<5 mm induration) during initial testing were retested 12 weeks later. TB disease was defined as clinical signs or symptoms of TB with bacteriologic or radiographic confirmation. Latent TB infection (LTBI) was defined as a positive TST result (>5 mm induration) and exclusion of TB disease by chest radiograph and sputum culture. Patients with a positive TST result who either had a previously documented negative TST result within the preceding 12 months or reported not having a previous positive TST were assumed to be recently infected by the HCW. As of August 2004, a total of 481 contacts had been identified; 48 (10%) were patients from other jurisdictions who had been referred for evaluation by TB-control programs in their jurisdictions. Of the remaining 433 contacts, 95 (22%) were employees, and 291 (67%) were patients of the dialysis center; an additional 47 (11%) were other contacts*. Of the 433 contacts, 333 (77%) were evaluated (Table); 36 (11%) had a previous positive TST result. The remaining 297 contacts received a TST; 48 (16%) had a positive TST result. A total of 41 (12%) of the 333 evaluated contacts reported TB symptoms, but TB disease was excluded by chest radiograph and sputum culture. The dialysis center employees were assumed to be immunocompetent and used as a surrogate group of contacts to evaluate for evidence of TB transmission. Of the 95 employees identified as contacts, 80 (84%) were evaluated; of these, 12 (15%) had a previously documented positive TST result. The remaining 68 employees received a TST; 13 (19%) had a positive TST result. Employees with positive TST results had chest radiographs that were normal. The 13 employees with a positive TST result were similar to the 55 employees with a negative TST result (i.e., by hours of exposure to the HCW, national origin, race/ethnicity, and age). Six (46%) of the 13 employees with a positive TST result had documented TST conversion (i.e., induration increase of >10 mm compared with a routine TST obtained during the 2-year period before exposure); four worked on the same shift as the HCW. No routine TB screening program had been conducted for patients at the dialysis center. One patient had a documented negative TST result before the exposure; 16 patients reported a previous positive TST result. Of the 291 patients identified as contacts, 212 (73%) were evaluated; 196 (92%) received a TST. A total of 76 (26%) had chest radiographs; five (7%) had abnormal radiographs, and TB disease was excluded subsequently by sputum culture. A total of 29 (15%) patients had a positive TST result. Patients with a positive TST result were older (median age: 65 years; range: 44--88 years) than those with a negative TST result (median age: 60 years; range: 11--95 years) (p = 0.01, Wilcoxon rank-sum). The median time of exposure to the HCW was the same (16 hours) for patients with positive and negative TST results. Of the 196 patients, 72 (37%) received direct care from the HCW; of these, nine (13%) had a positive TST result. Among the 72 patients, the median time of exposure was not different for those with a positive TST result compared with those with a negative TST result. Employees with a positive TST result and exposed patients were offered a twice-weekly 9-month regimen of isoniazid. As of September 10, six employees and six patients had completed treatment for LTBI, and two patients had died of unrelated causes while receiving treatment. Two patients are continuing LTBI treatment. No secondary cases have been identified. Reported by: L Hickstein, C McPherson, MD, D Kwalick, MD, V DeFriez, R Todd, DrPH, Nevada State Health Div. K Ijaz, MD, I González, MD, M Haddad, MSN, P Tribble, MA, Div of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention; M Arduino, DrPH, Div of Healthcare Quality Promotion, National Center for Infectious Diseases; S Wei, Div of Applied Public Health Training, Epidemiology Program Office; J Miller, MD, EIS Officer, CDC. Editorial Note:In this report, TST conversions among six immunocompetent employees suggest that M. tuberculosis transmission occurred within the renal dialysis center. Only one patient had a previously documented TST result for comparison; therefore, all 29 patients with a positive TST result were considered recently infected. Because exposure duration did not differ between the employees with positive TST results and those with negative TST results, no minimum level of exposure was associated with risk for infection with M. tuberculosis. The findings in this report are subject to at least one limitation. The majority of persons with chronic renal failure have impaired delayed-type hypersensitivity, which might result in false-negative TST results (3--5). The positive TST results from this investigation likely underestimated the true prevalence of LTBI among these patients. CDC recommends that after a known exposure to infectious TB disease, immunocompromised persons should receive treatment for presumptive LTBI, regardless of TST result (2). LTBI treatment was offered to all patients exposed to the HCW, even if their TST remained negative after repeat screening. However, convincing these high-risk contacts of the benefits of treating LTBI often was unsuccessful even after repeat counseling. Therefore, this investigation fell short of the national health objective for 2010 that 85% of TB contacts and other persons at high risk complete a course of treatment for LTBI (6). Because recently infected contacts are at high risk for having TB disease, the local health department is training the dialysis center employees to detect signs and symptoms of TB disease and ensure that anyone with TB symptoms is identified and treated promptly. If dialysis patients have TB disease diagnosed, maintenance dialysis in airborne isolation is required until they have completed enough anti-TB therapy to demonstrate clinical improvement and have negative M. tuberculosis sputum cultures. TB infection has a higher risk for progression to TB disease among renal dialysis patients because of their older age and immunocompromised status associated with chronic renal failure and other illnesses (7). Studies in New Jersey and California have documented TB disease rates six to 11 times greater among hemodialysis patients than among the overall state populations (8,9). Because these patients spend more time in health-care settings, when M. tuberculosis infection progresses to TB disease, they can expose other persons who also are at greater risk for disease. Therefore, despite the limitations of TST in this population, early detection and treatment of LTBI is imperative (2). All dialysis patients should be tested at least once for a baseline TST result and rescreened if TB exposure is detected (2,10). References
* Relatives of the HCW, persons who accompanied patients to the dialysis center, and persons with unidentified relationships to the HCW. Table 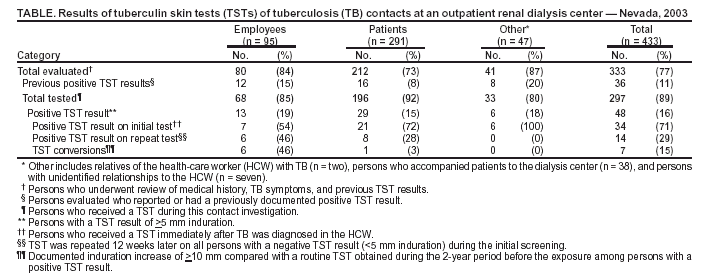 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/23/2004 |
|||||||||
This page last reviewed 9/23/2004
|