 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Aflatoxin Poisoning --- Eastern and Central Provinces, Kenya, January--July 2004In May 2004, CDC Kenya, trainees of the CDC-supported Field Epidemiology and Laboratory Training Program (FELTP) in Kenya, the World Health Organization, and CDC were invited by the Kenya Ministry of Health (KMOH) to participate in the investigation of an outbreak of jaundice with a high case-fatality rate (CFR) in the districts of Makueni and Kitui, Eastern Province. Preliminary laboratory testing of food collected from the affected area revealed high levels of aflatoxin, suggesting that the outbreak was caused by aflatoxin poisoning, as was a previous outbreak in the same area in 1981 (1). In the United States, aflatoxin concentrations are limited to 20 parts per billion (ppb), a level also adopted by Kenyan authorities. The 2004 outbreak resulted from widespread aflatoxin contamination of locally grown maize, which occurred during storage of the maize under damp conditions. Urgent replacement of the aflatoxin-contaminated maize with noncontaminated maize proved to be a critical intervention; however, as of July 21, a limited number of new cases continued to be detected. This report summarizes the preliminary results of the outbreak investigation. Aflatoxin poisoning likely will continue to be a public health problem until culturally appropriate storage methods for dry maize are implemented by the local population. In addition, enhanced surveillance for human aflatoxin poisoning and testing of commercially sold maize for aflatoxin levels will lead to long-term improvements in public health. Joint KMOH and CDC teams conducted patient interviews and reviewed medical records dating back to January 1, in three health facilities in the Makueni and Kitui districts. Additional case finding was conducted through similar patient interviews and retrospective record reviews in seven health facilities in adjacent districts of Eastern Province (Machakos, Embu, Mbeere, and Mwingi districts) and Central Province (Thika district) and at Kenyatta National Hospital in Nairobi (Figure 1). Large-scale active surveillance occurred from early May to late June. As of July 21, three health facilities in Makueni and Kitui districts continued to be monitored for new cases. A convenience sample of 20 patient households was visited to assess the occurrence of jaundice in nonhospitalized household members and to inspect food quality and storage. In this investigation, a case of suspected aflatoxin poisoning was defined as a case of acute jaundice that occurred after January 1, in a resident of Eastern or Central Province or a case diagnosed at Kenyatta National Hospital in a patient who was not known to have chronic liver disease or any other cause of jaundice. As of July 20, a total of 317 cases had been reported, with 125 deaths (CFR = 39%). An increase in case reports began in the third week of April, with new cases continuing to occur through mid-July (Figure 2). Of the 308 patients for whom age data were available, 68 (22.1%) were aged <5 years; 90 (29.2%) were aged 5--14 years, and 150 (48.7%) were aged >15 years. Of the 317 total patients, 178 (56.2%) were male, and 280 (88.3%) resided in four districts: Makueni (148 [46.7%]), Kitui (101 [31.8%]), Machakos (19 [6.0%]), and Thika (12 [3.8%]). The remaining 37 (11.7%) patients had aflatoxicosis diagnosed at Kenyatta National Hospital in Nairobi or at health facilities in Embu, Mbeere, or Mwingi districts. CFR was significantly higher in Makueni district (CFR = 49.3%) than in Kitui district (CFR = 23.7%) (CFR ratio = 2.1; 95% confidence interval [CI] = 1.4--3.1). Preliminary results from a case-control study that compared 40 case-patients with 80 well controls matched by village in Makueni and Kitui districts demonstrated a statistically significant association between the development of jaundice and several risk factors or markers, including 1) reported consumption of cooked maize kernels (odds ratio [OR] = 8.0; 95% CI = 1.7--37.1), 2) reported possession of homegrown maize that was discolored or visibly contaminated with mold (OR = 5.9; 95% CI = 1.9--18.2), 3) consumption of homegrown maize (OR = 3.0; 95% CI = 1.0--8.8), 3) storage of damp maize (OR = 3.5; 95% CI = 1.2--10.3), 4) inside storage of maize rather than outside granary storage (OR = 12.0; 95% CI = 1.5--95.7), and 5) reported deaths of dogs or livestock (OR = 3.3; 95% CI = 1.2--9.1). Food samples collected from household visits during May 10--19 included maize flour, maize grains, dry maize cobs, muthokoi (i.e., maize in which the outer hulls have been removed), millet, sorghum, and beans. A total of 31 samples were tested by the Kenya National Public Health Laboratory Services, and 15 had >20 ppb aflatoxin B1 (range: 20--8,000 ppb). A representative survey of maize products from agricultural markets and outlets (Figure 3) in Makueni, Kitui, Thika, and Machakos districts was conducted to assess the extent and magnitude of aflatoxin contamination in the sampled maize. Preliminary results indicated widespread, high-level aflatoxin contamination. A total of 182 (53.2%) of 342 samples had >20 ppb of aflatoxin. In addition, a substantial percentage of samples from each district had aflatoxin levels >1,000 ppb: Makueni (12.1%), Kitui (9.6%), Thika (3.9%), and Machakos (2.9%). The government of Kenya is providing replacement food in the most heavily affected districts: Makueni district (population: 771,545) and Kitui district (population: 515,422). Residents of affected districts have been advised to avoid consumption of maize or other foods suspected to be moldy or appearing discolored. In addition, food inspections by public health authorities are being conducted, and suspect food is being seized, destroyed, and replaced. Surveillance for possible aflatoxin poisoning in humans has been extended to other parts of Kenya by MOH, and aflatoxin screening of maize has been increased. Reported by: J Nyikal, A Misore, C Nzioka, C Njuguna, E Muchiri, J Njau, S Maingi, J Njoroge, J Mutiso, J Onteri, A Langat, IK Kilei, J Nyamongo, G Ogana, B Muture, Aflatoxin Task Force, Kenya Ministry of Health; P Tukei, C Onyango, W Ochieng, Kenya Medical Research Institute; C Tetteh, S Likimani, P Nguku, T Galgalo, S Kibet, A Manya, A Dahiye, J Mwihia, I Mugoya, Kenya Field Epidemiology and Laboratory Training Program/Kenya Ministry of Health. J Onsongo, A Ngindu, World Health Organization Kenya Country Office. KM DeCock, K Lindblade, L Slutsker, P Amornkul, D Rosen, D Feiken, T Thomas, CDC Kenya. P Mensah, N Eseko, A Nejjar, World Health Organization Regional Office for Africa. M Onsongo, F Kessel, Foreign Agricultural Svc, U.S. Dept of Agriculture. H Njapau, DL Park, Center for Food Safety and Applied Nutrition, Food and Drug Administration. Div of International Health, Epidemiology Program Office; L Lewis, G Luber, H Rogers, L Backer, C Rubin, National Center for Environmental Health; KE Gieseker, E Azziz-Baumgartner, W Chege, A Bowen, EIS officers, CDC. Editorial Note:Evidence that this outbreak resulted from aflatoxin poisoning included 1) high levels of aflatoxin (up to 8,000 ppb) in maize samples collected from patient households, 2) a clinical illness consistent with acute aflatoxin poisoning, 3) clustering of cases among residents of the same household, and 4) reports of deaths among animals known to have eaten the same maize as the patients during the same period. Serum specimens from a convenience sample of seven patients were tested for differential viral etiologies. All seven patients had negative serologic tests for yellow fever, dengue, West Nile virus, Rift Valley fever, Chikungunya and Bunyamwera viruses, acute hepatitis A, acute hepatitis B, and hepatitis C. Aflatoxins are a group of metabolic products formed by two species of fungus, Aspergillus flavus and A. parasiticus, in several agricultural commodities, including corn or maize. Two structural types of aflatoxins are known (B and G types), of which aflatoxin B1 is considered the most toxic and was the type most commonly found in Kenya during this outbreak. Exposure to aflatoxins occurs primarily through ingestion of contaminated foods (2) and can cause hepatic and gastrointestinal injury and have immunosuppressive, teratogenic, and oncogenic effects. Chronic low-level aflatoxin exposure can increase the risk for hepatocellular carcinoma (3). Severe, acute liver injury with high morbidity and mortality has been associated with high-dose exposures to aflatoxins (4). Ingestion of 2--6 mg/day of aflatoxin for a month can cause acute hepatitis and death (5,6). The largest reported outbreak of aflatoxicosis to date occurred in western India in 1974, resulting in 397 recognized cases and 106 deaths (6). The ongoing epidemic in Kenya already has resulted in 125 recognized deaths. Because of the remoteness of villages in the affected districts in Kenya and the large geographic area involved, case finding has been limited to medical facilities. In addition, because some persons might not have been able to reach health-care facilities for diagnosis and treatment, the true magnitude of this outbreak is likely to be considerably greater than reported. An outbreak of acute aflatoxicosis (20 cases; CFR = 60%) was reported previously in Makueni district, Eastern Province, Kenya, in 1981 (1). Patients were clustered in family groups that shared meals consisting of aflatoxin-contaminated maize (1,600--12,000 ppb). Acute hepatitis associated with consumption of moldy grains also has been reported in other areas in Africa, Western India, and Malaysia (6--8), where affected persons came from areas prone to drought and malnutrition and unseasonable rains forced the harvest of grains before adequate drying had occurred. Typically, increased reports of jaundice and hepatitis followed within weeks of such harvests (6--8). Locally produced maize associated with this outbreak was harvested in February during peak rains, and the first illnesses were reported in Makueni district in late March and early April. For every symptomatic case of aflatoxicosis identified, several other persons likely were exposed to unsafe levels of aflatoxin and might face future adverse health consequences. In addition, individual cases or clusters of aflatoxin poisoning likely occur regularly but are not recognized. Efforts should focus on the prevention of aflatoxin exposure by implementing extensive food replacement, without which, the epidemic can be expected to continue. Longer-term requirements include strengthened surveillance; increased food inspections to ensure food safety; and local education and assistance to ensure that maize is harvested correctly, dried completely, and stored properly. This report describes the first investigation by the Kenya FELTP, a partnership of CDC, KMOH, and Jomo Kenyatta University of Agriculture and Technology intended to build public health, epidemiologic, and laboratory capacity in Kenya. This investigation provided field experience to these Kenyan public health workers in training and exemplified collaboration between different national and international agencies and among various sectors and disciplines, including health, agriculture, food safety, nutrition, and humanitarian relief. Increased collaboration between the health sector and others involved in food security and safety could enable early warning of high levels of aflatoxins. As a result of widespread drought, Kenya faces an acute food shortage, with nearly 1.8 million persons in 26 districts vulnerable to food insecurity (9), including persons in the area most heavily affected by the aflatoxicosis outbreak. Because an estimated 166,000 metric tons of food will be required to meet the requirements of emergency and school feeding programs during August 2004--January 2005, public health officials should be vigilant to a possible wider aflatoxicosis outbreak resulting from the large-scale storage and distribution of certain emergency food supplies. Acknowledgments The findings in this report are based, in part, on contributions by Makindu Sub-District Hospital, Makueni district, Mutomo Mission Hospital, Kitui district, other health facilities, staff at the National Public Health Laboratory Svcs, Kenya. References
Figure 1 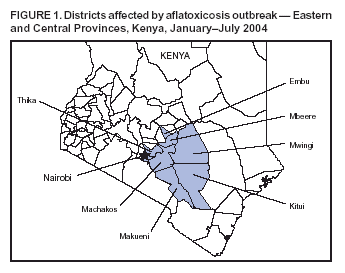 Return to top. Figure 2 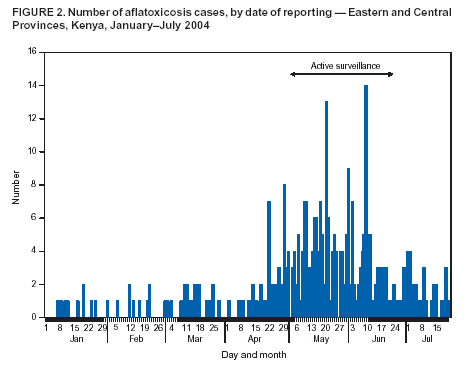 Return to top. Figure 3  Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/2/2004 |
|||||||||
This page last reviewed 9/2/2004
|