 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Suicide Among Hispanics --- United States, 1997--2001By 2020, Hispanics are expected to represent 17% of the U.S. population and to surpass all other racial/ethnic minority populations in size (1). In 1996, the U.S. Department of Health and Human Services established the Hispanic Agenda for Action initiative; a major goal of this initiative is to identify health problems that affect Hispanics (2). In 2001, although the overall age-adjusted suicide rate per 100,000 population among Hispanics (5.6) was lower than the U.S. national rate (10.7), suicide was the third leading cause of death among young (i.e., aged 10--24 years) Hispanics and the seventh leading cause of years of potential life lost before age 75 years (3). To identify demographic groups at risk for suicide and to help guide prevention efforts, CDC analyzed mortality data for 1997--2001. This report summarizes the results of that analysis, which indicated that, among Hispanics, the largest proportion of suicides occurred among young persons; suicide rates were higher among males; and the most common method of suicide was by firearms. To reduce the number of suicides, additional prevention strategies are needed, including 1) improving methods for collecting data about suicides, suicide attempts, and related behaviors; 2) expanding evaluation of prevention efforts aimed at reducing suicidal behaviors; and 3) examining how effective interventions can be modified for diverse and culturally specific populations. Data were obtained from CDC's National Center for Health Statistics Underlying Cause of Death Mortality file (3). Hispanic ethnicity included persons of Mexican, Puerto Rican, Cuban, Central and South American, and other/unknown Hispanic origins* (1). Data for 1997--1998 and 1999--2001 were based on External Cause of Injury codes from the International Classification of Diseases, Ninth (ICD-9)† and Tenth (ICD-10)§ Revisions, respectively (4). Suicide data for 1997--2001 were examined for the Hispanic population by sex, age group, and subpopulation. Suicide data for the most recent 3-year period available (1999--2001) also were examined by the three leading suicide methods: firearms (X72--X74), suffocation (X70), and poisoning (X60--X69). Population estimates for 1997--2001 from the U.S. Census bridged-race population estimates were used to calculate rates (5). The intercensal estimates used for 1997--1999 take into account the increase observed in this population between Census 1990 and Census 2000. Age-adjusted rates per 100,000 population were calculated on the basis of the 2000 U.S. standard population. Rates based on <20 deaths or with a coefficient of variation of >30% were considered unstable and therefore not reported. During 1997--2001, a total of 8,744 Hispanics (age-adjusted rate: 5.95 per 100,000 population) died from suicide; 7,439 (85%) were males. The age-adjusted rate for males was 5.9 times the rate for females (10.46 versus 1.78, respectively). Approximately 50% of all suicides occurred among persons aged 10--34 years, although the highest overall rate was among persons aged >85 years (Table 1). For Hispanic males, the suicide rate was highest among those aged >85 years, followed by those aged 80--84 years and those aged 75--79 years (36.54 versus 31.55 and 21.69, respectively). For Hispanic females, rates were highest among those aged 50--54 years, followed by those aged 45--49 years and those aged 15--19 years (3.12 versus 2.52 and 2.36, respectively). Persons of Mexican origin accounted for the majority of suicides (4,934 [56%]), followed by persons of other/unknown Hispanic origin (1,219 [14%]), Central and South Americans (950 [11%]), Puerto Ricans (932 [11%]), and Cubans (709 [8%]). Although rates could not be calculated for these subpopulations, the distribution of suicide was similar to the proportionate distribution of the U.S. Hispanic population by subpopulation (1). During 1999--2001, a total of 5,332 Hispanics died from suicide; 4,531 (85%) were males. Firearms were the suicide method reported most frequently (2,405 [45%]), followed by suffocation (1,834 [34%]) and poisoning (542 [10%]) (Table 2). Among Hispanic males, firearms were the most common suicide method (48%), followed by suffocation (35%) and poisoning (7%). In contrast, Hispanic females used firearms (29%), suffocation (29%), and poisoning (27%) each in similar frequency. Among Hispanic males aged 10--24 years (n = 1,135), firearms accounted for 52% of all suicides, followed by suffocation (38%) and poisoning (3%), whereas among females in the same age group (n = 211), suffocation accounted for 44% of all suicides, followed by firearms (33%) and poisoning (11%). Reported by: RM Ikeda, MD, A Crosby, MD, Div of Violence Prevention; RG Thomas, MSIM, JL Annest, PhD, Office of Statistics and Programming, National Center for Injury Prevention and Control; SI Berrios-Torres, MD, EIS Officer, CDC. Editorial Note:This report highlights the magnitude and demographics of Hispanic suicides, which occurred predominantly among males. Overall, firearms were the most frequently reported method used, although suffocation also was common among males and females. The findings in this report are subject to at least five limitations. First, because reporting of Hispanic ethnicity by all 50 states and the District of Columbia has been in effect only since 1997, the years for which complete data are available are limited. Second, although Census 2000 was the first to include a separate question on Hispanic origin in the Commonwealth of Puerto Rico, national statistics do not include its 3.4 million Hispanic residents (1). Third, during 1997--2001, rates could not be compared by geographic location because a large percentage (17 [33%]) of states had unstable rates. Fourth, unavailability of comparability ratios for individual method of suicide at the time of analysis precluded the ability to perform trend analysis or combine 1997--1998 and 1999--2001 data to examine further certain subcategories, such as mechanism of injury (6). Finally, numerator data on suicides by Hispanic subpopulations are available, but the corresponding denominator data are not available using the bridged-race population estimates, which precluded calculating age-adjusted rates or comparing rates between subpopulations. Although higher suicide rates were among older males, young Hispanics also are at risk. Hispanic youth are the fastest-growing segment of the U.S. population, accounting for 48% of the total Hispanic population and 26% of Hispanic suicides (versus 2% and 4% for Hispanics aged >75 years, respectively). Hispanics in grades 9--12, particularly females, report more feelings of sadness or hopelessness and of suicidal ideation and attempt, compared with their white or black non-Hispanic counterparts (7). Higher prevalence of these risk factors for suicidal behavior from previous studies and the high incidence of suicide among Hispanic youth reported in this study suggest that Hispanic youth should be targeted for self-harm prevention efforts. To intervene and prevent suicide successfully, organizations should apply the knowledge gained from studies on risk and protective factors. Risk- and protective-factor research focusing on Hispanic youth is limited. However, mental illness, substance abuse, acculturative stress, family dysfunction, and lower socioeconomic status have been associated with increased risk for suicidal behavior, and family support has been shown protective against suicidal behavior (8). Additional data are needed for comparison before definitive statements about similarities or differences across racial/ethnic categories and among Hispanic subpopulations can be made. Data about specific risk and protective factors in the Hispanic population (e.g., the effects of physical and mental health, immigration, acculturation, religious beliefs, substance abuse, and access to health care) also are necessary to develop culturally appropriate prevention and treatment programs. For example, one study focused on a predominantly Hispanic group of patients evaluated for suicide attempts in a hospital emergency department (9). In that study, staff training, outpatient therapy, family therapy, and a video explaining the treatment resulted in lower rates of suicide reattempts and suicidal reideation (9). To reduce the number of suicides, additional prevention strategies are needed, including 1) improving methods for collecting data about suicides, attempted suicides, and related behaviors; 2) expanding evaluation of prevention efforts aimed at reducing suicidal behaviors; and 3) examining how effective interventions can be modified for diverse and culturally distinct populations. Effective suicide-prevention strategies need not be specific to suicide, but can address factors that are associated but not unique to suicidal behavior. A comprehensive, strategic plan for suicide prevention should include multiple points for prevention, maximizing the likelihood of reaching persons in need. The National Strategy for Suicide Prevention, developed in collaboration with multiple federal, state, academic, and community partners, provides a framework for action to prevent suicide (10). Acknowledgments This report is based in part on data provided by D White, MS, K Webb, Office of Statistics and Programming, National Center for Injury Prevention and Control, CDC. References
* Central American: Costa Rican, Guatemalan, Honduran, Nicaraguan, Panamanian, Salvadoran, and other Central American (excludes Mexican); South American: Argentinean, Bolivian, Chilean, Colombian, Ecuadorian, Paraguayan, Peruvian, Uruguayan, Venezuelan, and other South American; and other/unknown Hispanic origin: Dominican (Dominican Republic), Spaniard, and all other Hispanic or Latino. † Codes E950--E959 for 1997--1998. § Codes X60--X84, Y87.0, and U03 for 1999--2001.
Table 1 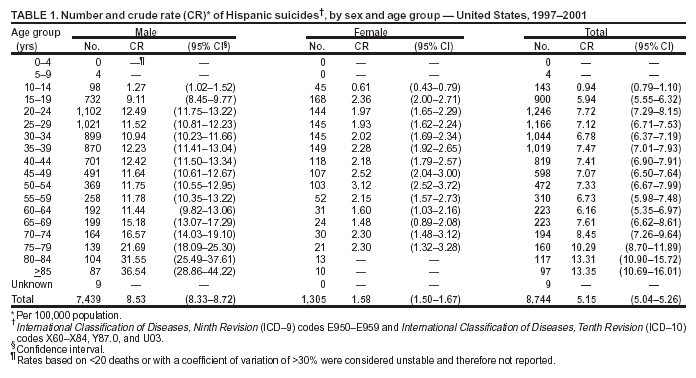 Return to top. Table 2 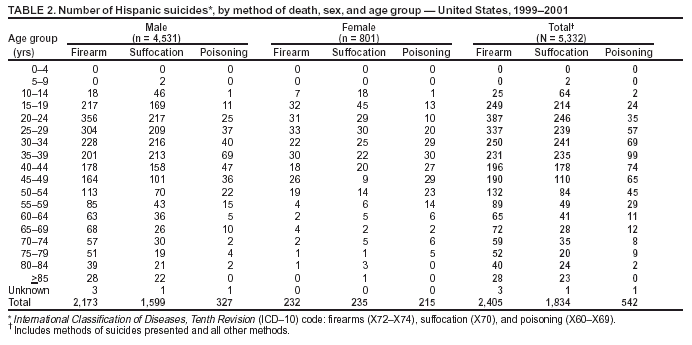 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 6/9/2004 |
|||||||||
This page last reviewed 6/9/2004
|