|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
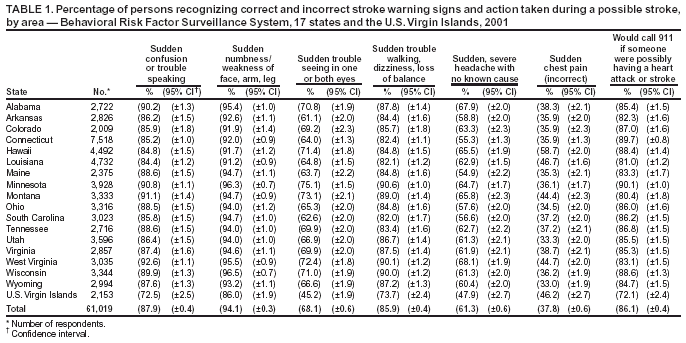
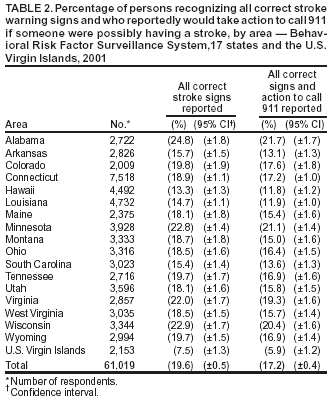
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Awareness of Stroke Warning Signs --- 17 States and the U.S. Virgin Islands, 2001Stroke is the third leading cause of death in the United States (1) and a major cause of disabilities among adults (2). Since 1900, the number of stroke deaths has declined (3), and substantial advances have been made in the diagnosis and treatment of ischemic stroke during the previous decade (4); however, the proportion of deaths that occur before patients are transported to hospitals has increased to nearly half of all stroke deaths (5). One of the national health objectives for 2010 is to increase the proportion of persons who are aware of the early warning symptoms and signs of stroke (objective no. 12.8) (6). To assess public awareness and knowledge of the proper emergency response, CDC analyzed 2001 data from the Behavioral Risk Factor Surveillance System (BRFSS) in 17 states* and the U.S. Virgin Islands (USVI). This report summarizes the results of that analysis, which indicated that public awareness of several stroke signs is high, but the ability to recognize the five major warning signs† is low. Education campaigns are needed to increase public awareness of stroke signs and the necessity of calling 911 when persons are suffering a possible stroke. BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized, civilian U.S. population aged >18 years. In 2001, the 17 states and USVI included a module in their surveys regarding symptoms of heart attack and stroke and the first action to take if someone were having a heart attack or stroke (7). The median response rate was 53.3% (range: 38.9%--70.8%). A total of 61,019 persons responded to questions about whether the following were warning signs of stroke: sudden confusion, trouble speaking or understanding; sudden numbness or weakness of face, arm, or leg; sudden trouble seeing in one or both eyes; sudden trouble walking, dizziness, or loss of balance or coordination; or sudden, severe headache with no known cause. An incorrect sign (i.e., sudden chest pain) was included to assess and account for the possibility that respondents would answer "yes" to all items in a series of closed-ended questions. Respondents also were asked to identify from the following the first action they would take if they thought someone was having a heart attack or stroke: take the person a hospital, advise the person to call a doctor, call 911, call a spouse or family member, or do something else. Data were weighted according to 2001 state population estimates. Prevalence estimates and 95% confidence intervals (CI) were calculated by using SUDAAN to account for the complex survey design. In 2001, public awareness of the major warning signs of stroke was high (Table 1). Signs recognized most commonly as someone possibly having a stroke were sudden numbness or weakness of the face, arm, or leg (94.1%); sudden confusion, trouble speaking or understanding (87.9%); and sudden trouble walking, dizziness, or loss of balance or coordination (85.9%). Signs least likely recognized as someone possibly having a stroke were sudden trouble seeing in one or both eyes (68.1%) and sudden, severe headache with no known cause (61.3%). Approximately 37.8% of respondents incorrectly reported sudden chest pain was a sign of stroke. A total of 86.1% of respondents reported they would call 911 if they thought someone was having a heart attack or stroke. Awareness of individual warning signs of stroke varied by state. The proportion of persons recognizing sudden, severe headache with no known cause as a warning sign ranged from 54.9% in Maine to 68.1% in West Virginia. In addition, the proportion of persons responding correctly that a 911 call was the first action to take if the respondent recognized signs that someone was possibly having a heart attack or stroke ranged from 80.4% in Montana to 89.7% in Connecticut. Recognition of the correct stroke warning signs (i.e., identifying the five major stroke warning signs and being aware that sudden chest pain was not a stroke sign) was low (19.6%) among respondents (Table 2). In addition, only 17.2% of persons were both aware of all correct stroke signs and reported that they would first call 911 if they thought someone was having a heart attack or stroke. Awareness of all correct stroke warning signs and calling 911 was lower in USVI (5.9%) than in the states (range: 11.8% [Hawaii]--21.7% [Alabama]). Reported by: JB Croft, PhD, KJ Greenlund, PhD, C Ayala, PhD, NL Keenan, PhD, ZJ Zheng, PhD, GA Mensah, MD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Immediate emergency transport to the hospital and timely appropriate care can reduce disability and death associated with stroke. The public should be aware of the major warning signs of stroke and take prompt action for a stroke patient. The findings in this report indicate that, in 2001, although recognition of several individual signs was high, recognition of all five major warning signs and the need to call 911 immediately for care was low. These estimates of stroke signs awareness and the need for urgent action suggest that state and local public health efforts must improve public awareness of stroke urgency if the 2010 national health objective (6) is to be achieved. State variations in public awareness might reflect past education efforts by some state health departments, the American Stroke Association, and the National Institute of Neurological Disorders and Stroke; however, greater efforts are needed. The findings in this report are subject to at least three limitations. First, BRFSS data are based on self reports and are subject to social desirability and recall biases. Second, using closed-ended questions with fixed responses resulted in higher estimates of stroke sign recognition than using open-ended questions in which a respondent provides an answer but no choices are available to prompt the respondent (8); therefore, these estimates for individual signs probably overestimate the true prevalence of awareness. Finally, BRFSS excludes households without telephones. Stroke is an emergency event requiring immediate action. Friends, relatives, and co-workers of persons at high risk (i.e., those with uncontrolled high blood pressure or a history of transient ischemic attacks, atrial fibrillation, diabetes, stroke, or heart attack) and the general public need to be aware of the major warning signs and be willing to call 911 for emergency help. Education efforts to increase public recognition of stroke warning signs can reduce delays in arriving at an emergency department (9). These educational messages should be promoted in community settings (e.g., health-provider offices, schools, and worksites) or on grocery bags, pharmacy bags, or billboards to increase public awareness of major stroke warning signs and action. References
† Sudden confusion, trouble speaking or understanding; sudden numbness or weakness of the face, arm, or leg, especially on one side of the body; sudden trouble seeing in one or both eyes; sudden trouble walking, dizziness, or loss of balance or coordination; and sudden, severe headache with no known cause.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/6/2004 |
|||||||||
This page last reviewed 5/6/2004
|