 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Strength Training Among Adults Aged >65 Years --- United States, 2001Strength training (also referred to as resistance training) enables adults to improve their overall health and fitness by increasing muscular strength, endurance, and bone density and by improving their insulin sensitivity and glucose metabolism (1). For older adults (i.e., persons aged >65 years), strength-training exercises are recommended to decrease the risk for falls and fractures (2) and to promote independent living (Figure) (3). The American College of Sports Medicine recommends that adults include strength training as part of a comprehensive physical activity program (1). A national health objective for 2010 is to increase to 30% the proportion of adults who perform, >2 days per week, physical activities that enhance and maintain muscular strength and endurance (objective 22-4) (4). To determine the percentage and characteristics of older adults who perform strength training consistent with this objective, CDC analyzed data from the 2001 National Health Interview Survey (NHIS). This report summarizes the results of that analysis, which indicated that approximately 12% of persons aged 65--74 years and 10% of persons aged >75 years met the strength-training objective. These findings underscore the need for programs that encourage older adults to incorporate strength training into their lives along with regular physical activity. NHIS consists of face-to-face interviews that collect information on health, health care, health behaviors, and related factors. The 2001 survey used a stratified, multistage probability sample representative of the U.S. civilian, noninstitutionalized population. The overall response rate among selected adults was 73.8% (5). Data were collected from 6,152 respondents aged >65 years, and SUDAAN was used to account for the complex sampling design and sampling weights. A total of 615 respondents were excluded because of missing data on height and weight, health status, physical activity levels, and demographic characteristics; the final sample size was 5,537. Respondents were asked, "How often do you do physical activities specifically designed to strengthen your muscles, such as lifting weights or doing calisthenics?" Respondents were categorized as meeting the national strength-training objective if they engaged in strength training >2 days per week (4). Multivariate logistic regression analysis was used to test for associations between meeting the strength-training objective and specific characteristics of the older adults. Models accounted for sex, age, race/ethnicity, education, marital status, body mass index (BMI), and self-reported health status. Respondents also were asked about their participation in leisure-time physical activities (e.g., exercise, sports, and physically active hobbies) and how often they engaged for >10 minutes in 1) vigorous activities that caused heavy sweating or large increases in breathing or heart rate and 2) light or moderate activities that caused only light sweating or slight or moderate increases in breathing or heart rate. On the basis of the frequency and duration of their reported activities, respondents were categorized consistent with the national health objective for physical activity (objective 22-2) (4) as "active" (i.e., engaging in moderate-intensity physical activity for >30 minutes, >5 days per week, or in vigorous-intensity physical activity for >20 minutes, >3 days per week), "insufficiently active" (i.e., active at less than recommended levels), or "inactive" (i.e., engaging in no physical activity). Approximately 11% of respondents aged >65 years reported that they engaged in strength training >2 days per week (Table 1). Women were less likely than men (odds ratio [OR] = 0.74; 95% confidence interval [CI] = 0.61--0.90) to meet the objective. The likelihood of meeting the objective declined with advancing age and increased with level of education. Respondents who were obese (i.e., BMI >30 kg/m2) were less likely (OR = 0.59; 95% CI = 0.45--0.77) than those of healthy weight to meet the objective. Those reporting fair or poor health were less likely (OR = 0.37; 95% CI = 0.26--0.51) to meet the objective than those in excellent health. Among older adults categorized as physically active, 24.7% engaged in strength training (Table 2). Persons categorized as inactive (OR = 0.13; 95% CI = 0.10--0.16) and persons categorized as insufficiently active (OR = 0.50; 95% CI = 0.40--0.62) were less likely to engage in strength training than persons in the physically active group. An estimated 5.6% of respondents met the national objectives for both physical activity and strength training. Reported by: J Kruger, PhD, DR Brown, PhD, DA Galuska, PhD, D Buchner, MD, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that, in 2001, the majority of older adults, including those who met the national objective for physical activity, did not engage in strength training. These results suggest the need for targeted programs to encourage certain older-adult populations (e.g., women and persons who are less educated, obese, or physically inactive) to increase strength training. These populations are similar to those previously identified among persons aged >18 years who were less likely to engage in weight lifting >2 days per week (6). During 1998--2001, the proportion of older adults who met the national objective for strength training increased from 10% in 1998 (4) to 12% in 2001 among those aged 65--74 years and from 7% (4) to 10% among those aged >75 years. However, these prevalences remained less than half the 2010 national target of 30% of the adult population. To increase strength training among older adults, programs should address multiple factors, including 1) increasing awareness of fitness benefits, 2) affordability, 3) physical limitations, 4) accessibility (e.g., transportation), and 5) fear of injury. Programs can be offered at places of worship, community centers, senior centers, schools, and fitness centers (7). Older adults also can perform strength training in their homes by using chair exercises as described in exercise guides, videos, and free information from the Internet (Box (3,8). The findings in this report are subject to at least three limitations. First, because the data are based on the self-reports of survey participants, errors in reporting might have affected prevalence estimates. Second, because respondents were not asked to provide details about their strength training (e.g., number of repetitions or number of muscle groups exercised), the quality of the strength training could not be evaluated. Finally, because the survey did not include persons living in institutions, the results might not be generalizable to all older adults. The majority of older adults, including even those physically active, are missing opportunities to improve their overall health and fitness through regular strength training. Because only 5.6% have met the national objectives for both physical activity and strength training, all older adults should be encouraged to incorporate both regimens into their lives. Additional information is available at http://www.nia.nih.gov/exercisebook. References
Table 1 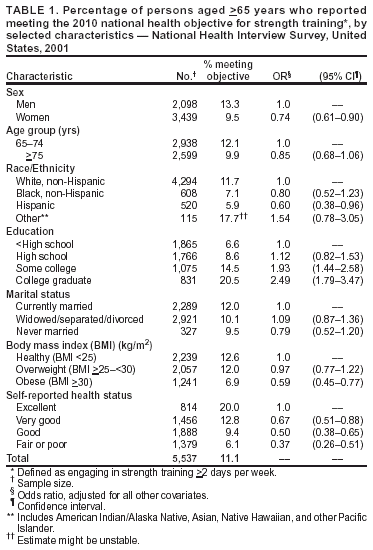 Return to top. Table 2 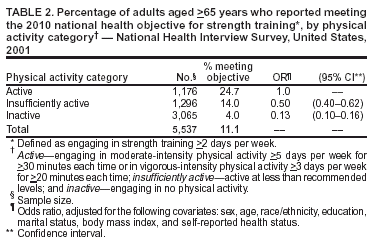 Return to top. Figure  Return to top. Box 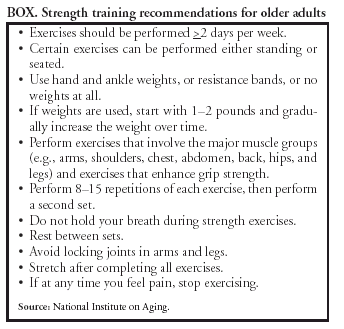 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 1/22/2004 |
|||||||||
This page last reviewed 1/22/2004
|