|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
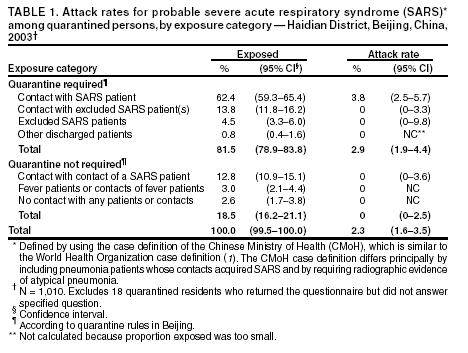
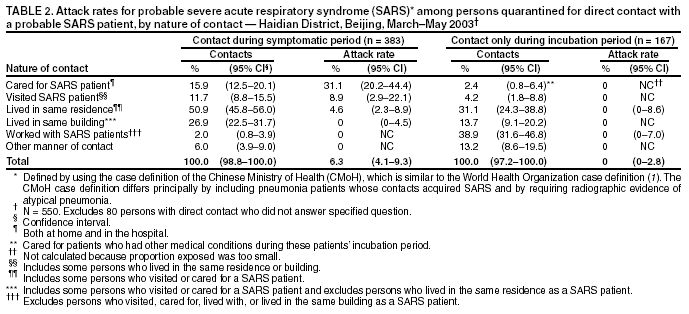
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Efficiency of Quarantine During an Epidemic of Severe Acute Respiratory Syndrome --- Beijing, China, 2003During March--July 2003, an epidemic of severe acute respiratory syndrome (SARS) in Beijing, China, accounted for 2,521 probable cases* (attack rate: 19 per 100,000 population). To control the epidemic, public health officials initiated enhanced surveillance, isolation of SARS patients, use of personal protective equipment (PPE) by health-care workers, and quarantine of contacts of known SARS patients. Approximately 30,000 Beijing residents were quarantined in their homes or quarantine sites. To guide future quarantine policy, the Chinese Field Epidemiology Training Program (China FETP) of the Chinese Center for Disease Control and Prevention (China CDC) conducted a survey to estimate the risk for acquiring SARS among quarantined residents of Haidian District (2001 population: 2.24 million), Beijing, in May 2003, 1 month after the epidemic peaked. This report summarizes the results of that survey, which indicate that, as a component of a comprehensive SARS-control program, quarantine should be limited to persons who have contact with an actively ill SARS patient in the home or hospital, allowing for better focus of resources in future outbreaks. The 33 precincts in Haidian District were divided into five locations: north (seven precincts), south (six), west (seven), east (six), and central (seven). From each location, the precinct with the greatest number of persons quarantined was selected based on lists from precinct quarantine officers. The selected precincts had 171 (29%) SARS cases and 1,210 (23%) persons quarantined in the district. Quarantined persons were asked to complete a self-administered questionnaire regarding the reasons for quarantine. Quarantined persons and their contacts were categorized as having SARS according to the criteria released by the Chinese Ministry of Health (CMoH). Persons with probable SARS on quarantine and surveillance lists for the precincts and the district were compared with surveyed persons to verify SARS in quarantined persons and their contacts. In Beijing, contact was defined as 30 minutes' exposure in the following situations to a SARS patient who required quarantine: 1) health-care workers who did not use PPE while evaluating or treating a SARS patient; 2) other persons (e.g., family members) who provided care for a SARS patient; 3) persons who shared the same living quarters as a SARS patient; 4) persons who visited a SARS patient; 5) persons who worked in the same office room or workshop as a SARS patient; 6) classmates or teachers of a SARS patient; and 7) persons using the same public conveyance as a SARS patient (rules varied by conveyance). Quarantine was for 14 days after exposure. Quarantine was initially for persons exposed to a SARS patient <14 days before the patient's illness onset, but this period was reduced to 10 and then to 3 days. Travelers who had fever (>100.4º F [>38º C]) arriving from other SARS-affected cities were placed under personal surveillance† instead of quarantine. All quarantined persons were followed up daily by a home visit or telephone call from the precinct quarantine officer and were given food and, if needed, medicine. If they acquired fever while under quarantine, they were transferred to a hospital for isolation. Some employers paid salaries to their employees under quarantine. In Haidian District, during March 1--May 23, a total of 5,186 persons (0.23% of 2.24 million residents) were quarantined. During May 26--June 4, a total of 1,210 residents were sampled; 1,028 (85%) completed the questionnaire. A total of 232 (2.3%; 95% confidence interval [CI] = 1.6%--3.5%) residents of the surveyed population (n = 1,010) acquired probable SARS while under quarantine (Table 1). The median quarantine period was 14 days (range: 1--28 days). Only quarantined persons who had a history of contact with a SARS patient acquired SARS during quarantine. In contrast, none of the quarantined persons whose exposure did not involve contact with a SARS patient acquired SARS; these included persons (e.g., a contact of a SARS contact or a contact of a patient with fever only) who had been quarantined mistakenly early in the outbreak before procedures were well known to all quarantine officers. In addition, as hospital isolation of persons under surveillance for SARS was relaxed, these persons required quarantine for potential exposure to an actual SARS patient in the hospital. Among the 626 (62%) quarantined persons with known contact with persons with probable SARS, those who cared for an actively ill SARS patient had the highest attack rate (Table 2). In contrast, quarantined persons who had contact with a SARS patient before they became ill had no detectable risk (95% CI = 0%--2.8%). In addition, no secondary transmission to relatives or other contacts was detected from persons who had SARS while under quarantine. No SARS patients detected through SARS surveillance reported a history of contact with a person under quarantine. Reported by: J Ou, Q Li, G Zeng, MSc, Chinese Field Epidemiology Training Program, Chinese Center for Disease Control and Prevention; Z Dun, A Qin, Haidian District Center for Disease Control and Prevention, Beijing, China. RE Fontaine, MD, Div of International Health, CDC. Editorial Note:Quarantine is the separation and/or restriction of movement of persons who, because of recent exposure to a communicable disease, risk acquiring that disease and subsequently exposing others. Estimates of the risk for acquiring disease are used to assess the efficiency of quarantine measures among persons with different types of exposure. The findings from this survey indicate that the efficiency of SARS quarantine could be improved greatly in future outbreaks. Focusing only on persons who had contact with an actively ill SARS patient would have reduced the number of persons quarantined by approximately 66%, without compromising its effectiveness. Persons exposed to SARS patients only during the incubation period appeared to have low or no risk for acquiring SARS (2,3). Because fever is a reliable marker for both onset of SARS and risk for transmission, persons in contact with a SARS patient could be placed under personal surveillance, with temperature taken daily or more frequently. If fever is detected within the 10-day incubation period of SARS, they could then be isolated. Such a modification of quarantine policy could reduce resources expended for quarantine, including time adults spend in quarantine. The findings in this report are subject to at least five limitations. First, the five selected precincts, although considered to be representative of Haidian District, were not a probability sample. Therefore, some selection bias might affect estimates of proportions in different exposure categories but would have a minimal effect on the estimated attack rates. Second, although exposure categories had estimated attack rates equal to 0, CIs for these estimates were too wide to determine if the actual rates differed from background or to suggest that persons in the exposure categories did or did not require special quarantine or control measures. Third, self-reported data are subject to recall bias and inaccurate reporting of reasons for quarantine. Fourth, because SARS cases were not laboratory-confirmed, some persons who were quarantined for exposure to another respiratory disease and some quarantined persons who had another respiratory disease might have been included. These two effects can counteract each other, and their magnitude would depend on the background incidence of other atypical pneumonias, which was probably very low relative to SARS. Finally, no information was available regarding the reasons for nonresponse, and some additional selection bias could result. However, because the nonresponse rate was relatively low, this effect should be minimal. Although the findings described in this report suggest that quarantine effectively eliminated the risk for transmission of SARS from quarantined persons to others in the community, they also reveal certain challenges with applying quarantine measures under field conditions. Certain persons who were quarantined in Beijing did not have illnesses consistent with the quarantine criteria. In addition, early in the outbreak, persons were quarantined who had been exposed to persons evaluated for SARS who were excluded later. Furthermore, these same excluded SARS patients required quarantine for exposure to a SARS patient while in the hospital. Although this was corrected as SARS was characterized, more uniform and careful application of quarantine criteria at the beginning of a SARS epidemic might further reduce the number of persons quarantined. The SARS attack rates in Beijing among all quarantined persons and special, well-defined exposure groups (i.e., persons treating or caring for a SARS patient, living in the same home with a SARS patient, or visiting a SARS patient) were approximately 10 times greater than those reported in a recent evaluation of SARS quarantine in Taiwan (4). Differences between the two outbreaks in the ratio of true SARS cases to SARS-like pneumonias from other causes, as well as differing classifications of exposure, could, in part, account for these findings. China FETP was initiated in October 2001 in the China CDC. China FETP also has training sites in several cooperating provincial CDCs. All 20 China FETP participants contributed substantially to the surveillance, investigation, and control of the 2003 SARS outbreak and completed five additional epidemiologic studies on SARS. The use of quarantine, in combination with enhanced surveillance, isolation of SARS patients, and comprehensive use of PPE by health-care workers, appears to have been effective in controlling the recent epidemic of SARS in Beijing. Limiting quarantine to persons who have contact with an actively ill SARS patient will likely improve the efficiency of quarantine and allow for better focus of resources in future outbreaks. References
* Defined by using the case definition of the Chinese Ministry of Health (CMoH), which is similar to the World Health Organization case definition (1). The CMoH case definition differs principally by including pneumonia patients whose contacts acquired SARS and by requiring radiographic evidence of atypical pneumonia. † Close medical or other supervision of contacts to permit prompt recognition of infection or illness but without restricting their movements (2).
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/30/2003 |
|||||||||
This page last reviewed 10/30/2003
|