|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
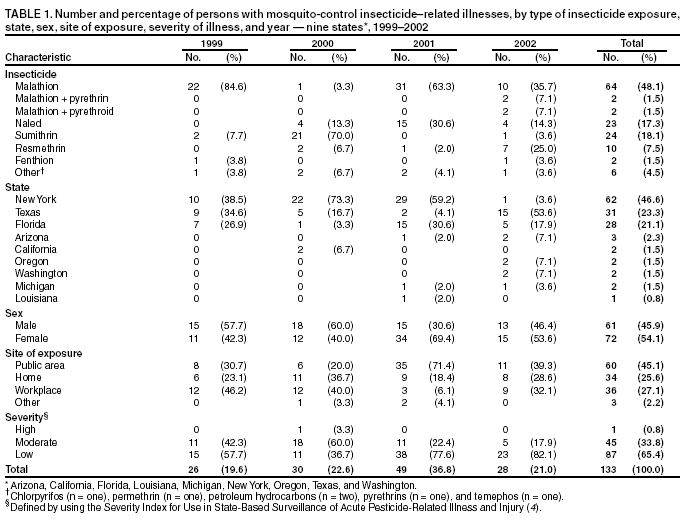
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Acute Insecticide-Related Illness Associated with Mosquito-Control Efforts --- Nine States, 1999--2002Ground and aerial applications of insecticides are used to control populations of adult mosquitoes, which spread such diseases as West Nile virus--related illness, eastern equine encephalitis, and dengue fever (1). This report summarizes investigations of illnesses associated with exposures to insecticides used during 1999--2002 to control mosquito populations in nine states (Arizona, California, Florida, Louisiana, Michigan, New York, Oregon, Texas, and Washington) (estimated 2000 population: 118 million). The findings indicate that application of certain insecticides posed a low risk for acute, temporary health effects among persons in areas that were sprayed and among workers handling and applying insecticides. To reduce the risk for negative health effects, public health authorities should 1) provide public notice of application times and locations and appropriate advice about preventing exposures, 2) ensure that insecticide handlers and applicators meet state-mandated training and experience requirements to prevent insecticide exposure to themselves and the public, and 3) implement integrated pest management control strategies that emphasize mosquito larval control, reduction of mosquito breeding sites, and judicious use of insecticides to control adult mosquito populations. Staff in state-based pesticide poisoning surveillance programs identified patients who had been exposed to insecticides used in mosquito-control efforts in nine states during April 1999--September 2002. Information was gathered on persons who had illnesses consistent with the national case definition for pesticide poisoning, which requires the collection of data on pesticide exposure, health effects, and toxicologic evidence supporting an association between exposure and effect (2,3). Cases of insecticide-related illness or injury were classified as either definite, probable, or possible, depending on the certainty of exposure and whether health effects were signs observed by a health-care provider or symptoms reported by a patient (2,3). Of the 133 cases of acute insecticide-related illness associated with mosquito control that were identified, two (1.5%) were classified as definite, 25 (18.8%) as probable, and 106 (79.7%) as possible. Of the 132 cases for which work-relatedness could be assessed, 36 (27.3%) were work-related and 96 (72.7%) were not work-related; 31 (86.1%) of the 36 work-related cases occurred among males, and 66 (68.8%) of the 96 cases that were not work-related occurred among females. Of the 49 cases identified in 2001, a total of 29 (59.2%) were related to a single event at a softball game in which workers operating a mosquito-control truck inadvertently sprayed 29 persons (16 spectators, 12 players, and one coach) with Fyfanon ULV®, which contains malathion. All 29 persons were treated in emergency departments (EDs). Of the 133 persons with acute insecticide-related illness associated with mosquito control, 35 (26.3%) were identified from monitoring media reports (including 34 reported subsequently by health-care providers), 32 (24.1%) were reported by poison-control centers, 27 (20.3%) were self-reported, and seven (5.3%) were reported by state health departments. Physicians and EDs were responsible for initial reporting of five and three cases, respectively. The remaining cases were reported initially by friends or relatives (n = seven), government agencies (n = five), employers (n = four), laboratories (n = two), and other sources (n = six). Of the 85 persons with reported illness who were known to have sought medical care, 45 (52.9%) were treated in EDs, 35 (41.2%) were treated in physicians' offices, four (4.7%) were treated in employee health centers, and one (1.2%) was hospitalized. An additional 16 persons received advice from a poison-control center, and 15 did not seek medical care; information about medical treatment was not available for 17 persons. Of the 133 reported cases of pesticide-related illness, 95 (71.4%) cases were associated with organophosphates, primarily malathion. Malathion alone was associated with 64 (67.4%) of the 95 cases; 37 (27.8%) cases were associated with pyrethoids, primarily sumithrin (24 cases) and resmethrin (10 cases) (Table 1). Illness severity was categorized for all cases (4). One exposure was associated with illness of high severity (Table 2). When her neighborhood was sprayed, a woman aged 54 years was exposed to sumithrin, which passed through operating window fans and a window air conditioner. She had exacerbation of her asthma and chronic obstructive pulmonary disease. The majority of the remaining cases were of low (65.4%) or moderate (33.8%) severity. The majority of cases were associated either with respiratory (66.2%) or neurologic (60.9%) dysfunction. Other systems affected were gastrointestinal (45.1%), ocular (36.1%), dermal (27.1%), cardiovascular (12.0%), renal-genitourinary (3.0%), and miscellaneous (28.6%). Of 36 persons who were exposed at their workplaces (Table 1), 14 (38.9%) were insecticide applicators, and 22 (61.1%) were performing tasks that did not involve pesticide application. Seven (50.0%) of 14 applicators were exposed to sumithrin; of the other 22 workers, 11 (50%) were exposed to malathion, and five (22.7%) were exposed to resmethrin. Illness of moderate severity was more frequent among applicators (42.9%) than nonapplicators (27.3%). Reported by: MP Mauer, DO, New York State Dept of Health. R Rosales, J Sievert, M Propeck, Texas Dept of Health. A Becker, MPH, Florida Dept of Health. E Arvizu, M Hadzizanovic, MD, Arizona Dept of Health Svcs. L Mehler, MD, California Dept of Pesticide Regulation. D Profant, PhD, C Thomsen, MPH, Oregon Dept of Human Svcs. L Baum, Washington State Dept of Health. M Lackovic, MPH, Louisiana Dept of Health and Hospitals. J Granger, MPH, Michigan Dept of Community Health. GM Calvert, MD, Div of Surveillance, Hazard Evaluations and Field Studies, National Institute for Occupational Safety and Health; WA Alarcon, MD, EIS Officer, CDC. Editorial Note:The findings in this report indicate that serious adverse outcomes potentially related to public health insecticide application were uncommon. When administered properly in a mosquito-control program, insecticides pose a low risk for acute, temporary health effects among persons in areas that are being sprayed and among workers handling and applying insecticides. In this analysis, adverse health effects were identified in a small percentage of the population in the nine states. Data about the actual number of persons potentially or actually exposed were not available because insecticide applications were conducted only in certain areas of participating states, and the boundaries of these areas were not available. Malathion, naled, sumithrin, and resmethrin were associated with the majority of reported cases of acute insecticide-related illness. Malathion is an organophosphate insecticide that is classified as an acute toxicity category III compound*. Although it is less acutely toxic than many other organophosphates, adverse health effects have been reported by exposed persons (5). Naled is an acute toxicity level I organophosphate. When combined with piperonyl butoxide, resmethrin and sumithrin are highly effective insecticides that are of low-order toxicity to mammals, including humans; these pyrethroid products are classified as acute toxicity category III compounds and have been associated with adverse health effects in humans (6,7). These insecticide formulations are registered by the U.S. Environmental Protection Agency for use in urban areas for mosquito control and benefit the public by controlling populations of mosquitoes that transmit diseases that affect humans. Reported symptoms associated with these insecticides were temporary and included dermal, ocular, and upper and lower respiratory tract irritation and exacerbation of conditions such as asthma. These health effects might represent irritant or allergic responses, to either the insecticide or its carrier (5,7,8). Anxiety about insecticide use for mosquito control also might have been responsible for symptoms in some persons. The findings in this report are subject to at least three limitations. First, the number of reported cases is probably an underestimate of the true magnitude of illnesses associated with mosquito-control efforts. Affected persons who did not seek medical care or whose symptoms were not reported to a surveillance system could not be identified; even if these persons had sought medical care, their illness might not have been recognized as insecticide-related, and even if they had received a proper diagnosis, their cases might not have been reported. Second, only nine states have pesticide poisoning surveillance systems, and the data in this report might not be representative of the 41 states without such surveillance systems. Finally, although all cases were consistent with case definition criteria, the possibility of false positives cannot be excluded. Because clinical findings of pesticide poisoning are nonspecific, especially when of mild severity, and no standard diagnostic test exists, some illnesses related temporally to insecticide exposures might be coincidental and not caused by the exposures. To reduce potential risks from insecticide exposure, CDC recommends the use of integrated pest management strategies for mosquito-control programs that emphasize mosquito larval control, reduction of breeding sites (e.g., human-made collections of stagnant water such as unchlorinated swimming pools, discarded tires or other containers, and bird baths), and judicious use of insecticides to control adult mosquito populations when quantitative measures suggest an elevated risk for human infection or in community settings when extensive immature mosquito larval habitats cannot be controlled (9,10). When insecticides are used, public health agencies should inform the public when and where spraying will occur and communicate how to reduce the likelihood of exposure. To avoid direct exposure from passing spray trucks, public health agencies should ensure that visible and audible warnings are made before spraying. Persons with exposure-related health concerns should consult their health-care providers. To prevent exposures from improper application methods, insecticide handlers and applicators should be trained in proper insecticide handling and application methods and in the use of appropriate personal protective equipment. References
* The U.S. Environmental Protection Agency classifies pesticide products into one of four acute toxicity categories on the basis of certain criteria, with category I comprising pesticides with the greatest toxicity and category IV those with the least toxicity. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/10/2003 |
|||||||||
This page last reviewed 7/10/2003
|