|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
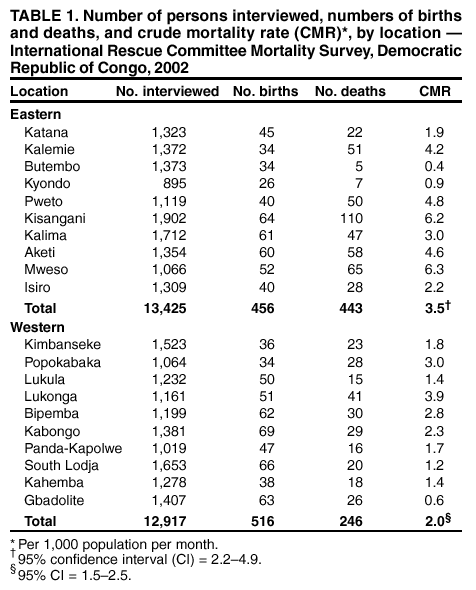
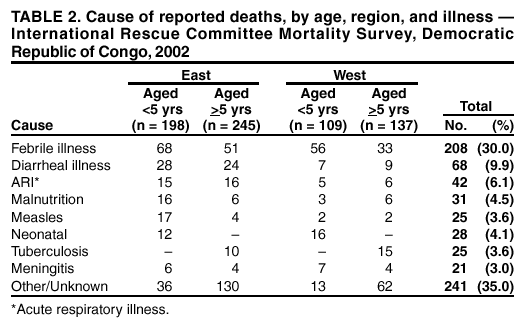
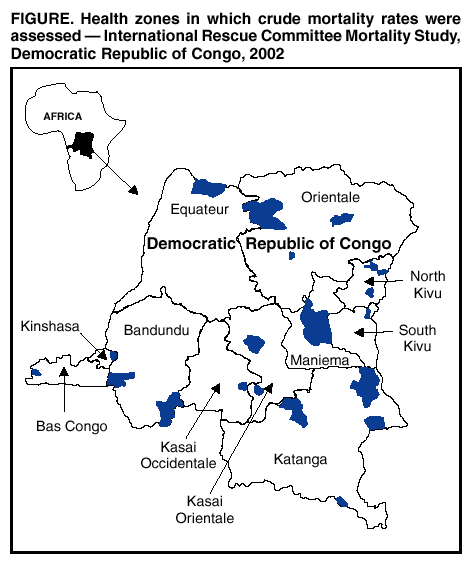
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Elevated Mortality Associated With Armed Conflict --- Democratic Republic of Congo, 2002In August 1998, citing a need to control insecurity on their western borders, Rwanda and Uganda sent troops into the Democratic Republic of Congo (DRC) (estimated 2002 population: 51 million). Within 6 months, troops from seven neighboring countries were fighting in the DRC, with various Congolese groups supporting different invading armies (1). During 1998--2002, the majority of the fighting occurred in the DRC's five eastern provinces (1996 population: 19.9 million). To assess the impact of the armed conflict on public health, the International Rescue Committee (IRC), with support from CDC, conducted a nationwide mortality survey to measure DRC's nationwide crude mortality rate (CMR) and to compare CMRs in DRC's five eastern provinces with CMRs in the five western provinces. This report summarizes the results of the survey, which indicate that the overall CMR in the DRC is the highest in the world, with the majority of deaths caused by preventable infectious diseases. The findings underscore the importance of the ongoing peace process, which appears to have contributed to a decrease in mortality rates in eastern DRC, and highlights the importance of collecting population-based health data regularly during armed conflicts. Conducted during September 14--November 13, 2002, the survey employed a three-stage cluster approach to measure CMRs. In the first stage, 20 health zones were selected systematically proportional to the population: 10 in the war-affected areas of the five eastern provinces (Katanga, Maniema, North Kivu, Orientale, and South Kivu) and 10 in the five western provinces (Bandundu, Bas Congo, Equateur, Kasai Occidentale, and Kasai Orientale) (Figure). Of approximately 14.3 million persons in the war-affected areas of the five eastern provinces, 5 million (35%) could not be visited because of ongoing fighting, and the health zones in which these persons live were excluded from the site selection process. All health zones in the five western provinces were available for selection. In the second stage, 15 locations were selected in each targeted health zone, with the probability of selection proportional to population; the locations comprised the smallest known population units (i.e., specific avenues, clinic areas, or villages). In the final stage, a specific household was selected by using one of three methods: 1) counting all households in the selected population and selecting one at random; 2) dividing the selected population into roughly equal segments, selecting one segment at random, counting the households in that segment, and selecting one at random; or 3) selecting a random point in space by using a map and a global positioning system unit if the population was spread over an entire clinic area with no further population breakdown. Interviewers visited the selected households and explained the purpose of the survey to a person aged >14 years. A person consenting to an interview was asked about the age and sex of current household residents and the occurrence of any pregnancies, births, or deaths among current residents since January 2002. From households selected initially, interviewers visited the next 14 closest occupied households. If no person aged >14 years was home, or if members of a household refused to be interviewed, the household was skipped and the next was visited. Persons were included as household residents only if they had slept in that household on the preceding night. CMRs were calculated by using the following formula: CMR = (number of deaths / number of living residents minus half the number of births plus half the number of deaths) x 1,000 / the number of months in the recall period. Deaths were included if a decedent had slept in the interviewed household or lived with the interviewed family at the time of death during 2002. The recall period was January 1, 2002, through the median day of the specific health zone evaluation (median: 9.3 months; range: 8.5--10.3 months). The mortality rate for children aged <5 years (<5MR) was estimated by using the following formula: <5MR = (number of deaths among children aged <5 years/number of children aged <5 years who were alive at the time of the survey plus one half of deaths among those aged <5 years during recall period) x 1,000 / the number of months in the recall period. This equation assumes that both the total number of children born and the number of children who turned age 5 years remained constant during the recall period. Mortality in this survey was expressed as deaths per 1,000 population per month. Previous findings indicate that a baseline CMR of 1.5 deaths per 1,000 population per month occurs in poor areas of sub-Saharan Africa in the absence of armed conflict (2). No person aged >14 years was present at the time of the survey in 488 (17.9%) of 2,717 households visited in the east and in 672 (23.0%) of 2,927 households visited in the west. Of 4,484 households in which a person aged >14 years was present at the time of the survey, 4,475 (99.8%) agreed to participate, and nine (0.2%) declined. Of the 10 selected eastern health zones, two could not be surveyed, one because of the refusal of local authorities and one because of security constraints. In each case, the closest neighboring health zone was surveyed. Of the 150 locations selected among the 10 eastern health zones visited, five (3.0%) were not surveyed because of time and logistic constraints, and five (3.0%) could not be reached for security reasons; if a location could not be reached, the nearest accessible village was visited instead. All 10 selected western health zones were surveyed, and all 150 locations were reached. During January--September 2002, CMR in the eastern provinces was 3.5 deaths per 1,000 population per month (95% confidence interval [CI] = 2.2--4.9), and the <5MR was 9.0 (95% CI = 4.0--14.0); the CMR in the western provinces was 2.0 (95% CI = 1.5--2.6), and the <5MR was 4.4 (95% CI = 3.2--5.7) (Table 1). These differences were not statistically significant. Cause of death was reported by interviewed families (Table 2). Of 689 reported deaths, 404 (59%) were attributed to infectious diseases, which also might have been responsible for other deaths for which the cause was reported as unknown. War-related violence accounted for no deaths in the west and for seven (1.6%) of 443 deaths reported in the east, compared with 69 (11.1%) of 624 violent deaths recorded by IRC in 2000 and 84 (9.4%) of 894 violent deaths in 2001 (3). On the basis of these results, the nationwide CMR is 2.2 deaths per 1,000 population per month, which exceeds the CMRs reported for all other nations in 2001 (4). If mortality among the approximately 5 million inaccessible persons who were not surveyed in the eastern provinces is at least as high as that in the areas surveyed, the nationwide CMR is approximately 2.4 deaths per 1,000 population per month. Reported by: L Roberts, PhD, M Zantop, MPH, International Rescue Committee, New York, New York. P Ngoy, MD, International Rescue Committee, Kinshasa; C Lubula, L Mweze, International Rescue Committee, Bukavu, Democratic Republic of Congo. C Mone, MPH, International Rescue Committee, Bujumbura, Burundi. Editorial Note:The nationwide CMR estimate for the DRC of 2.2 deaths per 1,000 population per month presented in this report is much greater than the 1.3 deaths per 1,000 population per month reported in 1997, the year before the outbreak of war (4). As is usually the case in protracted war settings, violence was not reported as the major cause of death (2). In both the war-affected and the nonwar-affected areas surveyed, febrile illness and diarrhea associated with infectious diseases were the most commonly reported causes of death. This might reflect deteriorating economic and health conditions combined with the disruption of the health-care system. During January 1999--August 2001, three nongovernment organizations recorded substantially elevated CMRs through population-based sample surveys of specific health zones with populations ranging from 62,000 to 347,000 persons. During January--August 2001, Doctors Without Borders documented CMRs of 1.2--9.0 deaths per 1,000 population per month in five health zones in five provinces (5). During 1999--2001, IRC conducted 11 surveys in seven health zones in the five eastern provinces. These surveys, with recall periods of 14--17 months, documented CMRs of 2.7--12.1 deaths per 1,000 population per month (3). Through an extrapolation process, these two IRC surveys were used to estimate an average CMR of 5.4 deaths per 1,000 population per month in the five eastern provinces during August 1998--April 2001 (3). Medical Relief International (MERLIN) documented a CMR of 10.0 deaths per 1,000 population per month in the eastern health zone of Kalima in a 3-month period during 2000 (MERLIN, unpublished data, 2001). Although the method of selecting health zones was not random in the two previous IRC surveys, by chance, two Eastern provinces (Kalima and Kalemie) were selected in both 2001 and 2002 and were evaluated during both years by using similar methods. The CMR in Kalima declined from 7.1 deaths per 1,000 population per month during January 2000--March 2001 to 3.0 during 2002. During the same period, the CMR in Kalemie declined from 10.8 deaths per 1,000 population per month to 4.2. The improved CMR reflects a decline of 96% in the rate of violent deaths, from 1.0 deaths per 1,000 population per month in 2000 to <0.1 in 2002. These findings for the eastern provinces indicate a marked reduction in CMRs during 2002 compared with the preceding 3 years (3). The findings in this report are subject to at least four limitations. First, avoiding areas with the worst security conditions probably resulted in underestimating CMRs. Second, data from past surveys conducted by IRC might not be comparable because different methods were used to select health zones. Third, because empty households experienced more deaths than occupied households (6), CMRs probably were underestimated. Finally, no formal verbal autopsy procedure was followed, and no independent confirmation of the deaths was sought. Violence-related mortality in eastern DRC has decreased when peace initiatives have been implemented. A peace accord signed in early 2001 curtailed hostilities substantially and resulted in the withdrawal of most foreign troops during 2002. In addition, during 2000--2002, approximately 5,500 United Nations (UN) observers arrived in addition to an increase in humanitarian assistance and aid workers. Epidemiologists can provide timely and representative health data to assess the public health impact of armed conflict. After the first series of IRC surveys conducted in 2000, the UN Security Council passed a resolution demanding the withdrawal of foreign troops (7). The impact of the second round of IRC surveys conducted in 2001 on the current peace process is unclear. Epidemiologic techniques involving creative, flexible, and practical measurement techniques need to be developed further and employed on a regular basis to address the public health consequences of armed conflicts. Humanitarian efforts in DRC should focus on the war-affected eastern areas and on controlling infectious diseases. References
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/22/2003 |
|||||||||
This page last reviewed 5/22/2003
|