|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
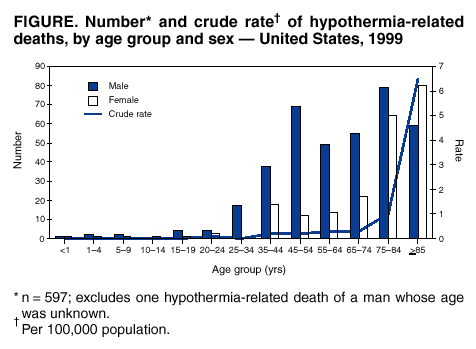
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hypothermia-Related Deaths --- Philadelphia, 2001, and United States, 1999Hypothermia is defined as the unintentional lowering of the deep body (core) temperature below 95.0º F (35.0º C). Hypothermia can be mild (90.0º F--<95.0º F [32.2º C--<35.0º C]), moderate (82.5º F--<90.0º F [28.0º C--<32.2º C]), or severe (<82.5º F [<28.0º C]). Common risk factors for hypothermia include exposure to cold while under the influence of alcohol or drugs, altered mental status, and immersion in cold water (1). During 1979--1998, approximately 700 persons (range: 420--1,024) died annually in the United States from hypothermia; approximately half of these deaths were attributed to extremely cold weather (2). This report presents three cases of hypothermia-related deaths in Philadelphia during 2001 as examples of risk factors for hypothermia and summarizes information about hypothermia-related deaths in the United States during 1999. Hypothermia deaths are preventable; by avoiding hypothermia, persons also can prevent other adverse health effects of cold weather. Case ReportsCase 1. In January 2001, a man aged 60 years was found dead by police; he was lying on a sofa inside an abandoned house that had no heat or electricity. Other inhabitants in the house reported that the man had been drinking alcohol before his death. During the 24 hours before the man was found, the minimum temperature was 21.0º F (-6.0º C). On autopsy, the man was found to have a blood alcohol concentration (BAC) of 0.23 g/dL; in Pennsylvania, drivers are considered intoxicated if their BAC is >0.10 g/dL. Case 2. In January 2001, paramedics were called to assist a man aged 25 years who was found unresponsive on a sidewalk late at night. The low temperature during the previous 24 hours was 31.0º F (-0.6º C). The man was transported to a hospital, where he was resuscitated through advanced cardiac life support protocol. He remained in a vegetative state and died 9 days later. His BAC at the time of admission was 0.48 g/dL; the underlying cause of death was listed as acute alcohol intoxication, with hypothermia as a contributing factor. Case 3. In February 2001, a woman aged 48 years was found collapsed along a roadside. During the previous day, approximately 2 inches of snow had fallen, and the minimum ambient temperature had been 29.0º F (-1.6º C). After transport to a hospital, her core body temperature was 91.5º F (33.0º C). The woman died despite extensive efforts at resuscitation, including intravenous infusion and peritoneal lavage with warmed fluids. Autopsy revealed bilateral pneumonia and positive blood toxicology for morphine and diphenhydramine. Sepsis was listed as the primary cause of death, with hypothermia as a contributing factor. United StatesSince 1999, CDC's National Center for Health Statistics (NCHS) has used information from death certificates categorized with International Classification of Diseases, Tenth Revision (ICD-10) codes to estimate national mortality trends. During 1999, exposure to excessive natural cold (ICD-10 code X31) was listed as the underlying cause of death (i.e., the circumstance of the accident that produced the fatal injury) for 598 persons in the United States (Figure), and hypothermia (ICD-10 code T68) was listed as a nature of injury (i.e., an injury that occurred to the decedent) in 1,139 deaths (2). Of the 598 hypothermia-related deaths, 380 (64%) occurred among males, and 359 (60%) of the 597 persons who died of hypothermia and whose age was known were aged >65 years. During 1999, Pennsylvania and New York had the greatest number of hypothermia-related deaths (36 each) (2), and Alaska had the highest crude death rate (1.9 per 100,000 population), approximately twice that of Montana, which had second-highest rate (0.9). Reported by: H Mirchandani, MD, Medical Examiner's Office; C Johnson, MD, Div of Disease Control, Philadelphia Dept of Public Health, Pennsylvania. Div of Environmental Hazards and Health Effects, National Center for Environmental Health; C Newbern, PhD, C Sanchez, MD, EIS Officers, CDC. Editorial Note:Hypothermia is an important cause of preventable deaths in the United States, especially among persons who abuse alcohol (3). Ethanol causes vasodilation, which produces a brief "warming" sensation that interferes with peripheral vasoconstriction, the physiological defense against cold, while also inducing hypoglycemia. Alcohol consumption in cold surroundings is a dangerous practice. Unattended children and persons aged >65 years also are at greater risk for hypothermia (3). Hypothermia during cold weather is the result of decreased heat production, increased heat loss, or impaired thermoregulation (1). Older persons, who have a decreased basal metabolic rate, might be at further risk for hypothermia because of impaired physical exertion, which produces heat to keep the body warm (4). Inactivity limits heat production through physical exertion, but overexertion can increase evaporation from the respiratory tract and cause fatigue. Shivering also can cause enough lactate generation eventually to produce acidosis and fatigue. Exposure to high winds can further increase heat loss. As body temperature decreases, the hypothalamus fails to compensate body temperature, and the central nervous system follows the progressive systemic depression of metabolism. Finally, metabolic impairment from alcoholism, malnutrition, hypothyroidism, or advanced age can cause poor endurance to cold (4). Warning symptoms for hypothermia in adults include shivering, confusion, memory loss, drowsiness, exhaustion, fumbling hands, and slurred speech. In children, symptoms include bright red, cold skin and extreme low energy (5). Immersion in warm water is highly efficient in raising body temperature but might hinder cardiopulmonary resuscitation (CPR) and more invasive techniques if needed. Drinking warm, nonalcoholic beverages can help raise body temperature if the person is conscious (5). However, none of these procedures substitutes adequately for proper medical attention, and special care should be taken when handling and transporting a patient because skin can become numb and slough easily. In the presence of severe hypothermia with cardiac arrest, CPR should be initiated on site and continued during transportation (5). Because of the protective effect that a low temperature might have on brain ischemia (especially if asphyxia has not preceded circulatory arrest), attempts at rewarming victims with severe hypothermia and cardiac arrest outside the hospital are not recommended (6). Core body temperature before rewarming might not be a good predictive factor for positive outcome, and persons with a core temperature as low as 59.0º F (15.0º C) have survived (1). The time between rescue and rewarming does not predict outcome (1); in the most extreme case, a boy aged 5 years recovered without apparent cerebral sequelae after 40 minutes of submersion in ice-cold water (7). Overall death rates from all causes increase during winter (3); in addition to hypothermia, cold temperature is associated with excess mortality from ischemic heart disease (8) and cerebrovascular disease (9). Cold-induced vasoconstriction and later hemoconcentration can result in rupture of atheromatous plaques and arterial thrombosis. Cold temperature also can lower the immune system's resistance to respiratory infection, causing an increase in respiratory disease mortality (9). Hypothermia-related morbidity is not exclusive to cold northern climates. Persons from regions with warmer winters might be at greater risk from the indirect effects of cold weather than persons from regions with colder and longer winters (9,10). However, geographic distributions might represent not only seasonal temperature variations but also socioeconomic status (which can limit access to controlled indoor temperature), cultural backgrounds (which can influence behavior toward individual protection from cold as well as outdoor activity), or populations with a higher proportion of elderly persons (10). Persons should take precautions to maintain body temperature both inside and outside during cold weather by heating the home (taking care to avoid carbon monoxide intoxication), especially at night, and by wearing properly insulated clothes while performing outdoor activities. The outer layer of clothing should be tightly woven and wind resistant. Inside layers of wool, silk, or polypropylene are preferred over cotton. Persistent shivering always is a signal to return indoors. References
Figure
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 2/6/2003 |
|||||||||
This page last reviewed 2/6/2003
|