 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Impact of September 11 Attacks on Workers in the Vicinity of the World Trade Center --- New York CityIn January 2002, CDC's National Institute for Occupational Safety and Health received requests for Health Hazard Evaluations from labor unions representing workers employed in buildings in the vicinity of the World Trade Center (WTC). Workers reported persistent physical and mental health symptoms that they associated with exposures from the WTC collapse and ensuing fires. To address these concerns, CDC conducted surveys of workers at four workplaces in New York City (NYC), a high school (high school A) and college (college A) near the WTC site, and a high school (comparison high school B) and college (comparison college B) >5 miles from the WTC site to determine rates of physical and mental health symptoms. This report summarizes the preliminary results of the employee surveys, which indicated that workers employed near the WTC site had significantly higher rates of physical and mental health symptoms than workers employed >5 miles from the site. Intervention programs should be tailored to address the needs of these workers, and the effectiveness of these programs should be evaluated. Further assessment is warranted to describe the nature and extent of illness in specific working groups and individual medical follow-up in those with persistent symptoms. CDC conducted site visits and distributed self-administered questionnaires in January 2002 to staff at high school A (n=224) and comparison high school B (n=155), and in March 2002, to staff at college A (n=374) and comparison college B (n=204). Teaching, administrative, support, and noncontract staff were included in the survey. Respondents were asked about work duties, mental health and physical symptoms after September 11, past medical history, and activities related to events at the time of the WTC terrorist attacks. Questions about physical symptoms were based on presumed types of exposures and employee concerns. Persons responding affirmatively to "Have you had any of the following symptoms after the WTC disaster on 9/11/01?" were defined as having symptoms. Physical symptoms included eye irritation, nose/throat irritation, cough, shortness of breath, chest tightness, wheezing, nausea, and indigestion. Persistent physical symptoms were defined as either 1) symptoms that existed before September 11 but worsened after September 11, or 2) new symptoms that developed after September 11 and had not improved. To assess mental health symptoms, the Center for Epidemiologic Studies Depression Scale (1) was used to define symptoms consistent with major depression. The Veteran's Administration post-traumatic stress disorder (PTSD) checklist (2) was used to determine prevalence of PTSD. Participation rates were 83% for high school A, 84% for high school B, 59% for college A, and 50% for college B. Staff at all four workplaces were similar by age, sex, race, education, and cigarette smoking status. On September 11, approximately 40% of high school A and 31% of college A staff saw an airplane crash into the WTC; 50% and 44%, respectively, witnessed the WTC collapse. In all four workplaces, 30%--40% of the respondents knew someone who was injured seriously or killed during the disaster. College A reopened for staff on September 26, and high school A staff returned to their building on October 20. Both buildings were within two blocks of the still burning WTC site and adjacent to a barge operation carrying the debris to the landfill site outside Manhattan. Approximately one fourth (27%) of staff at high school A and college A lost time from work because of physical symptoms experienced after the WTC disaster, compared with 14% at high school B (p<0.003) and 16% at college B (p<0.004). Compared with staff at high school B and college B, staff at high school A and college A reported a significantly higher prevalence ratio of new physician-diagnosed PTSD after September 11, but rates for allergies, asthma, and depression were not statistically different. Prevalence of eye irritation, nose/throat irritation, cough, nausea, and shortness of breath was significantly higher (p<0.05) for staff at high school A and college A, compared with staff at high school B and college B after September 11 (Table 1). Approximately 4--6 months after the attacks, 5%--30% of employees in high school A and college A had persistent physical symptoms (Table 2); the majority of these symptoms were significantly higher (p<0.05) in high school A and college A than in the comparison schools. Approximately one third (33%) of high school A and 24% of college A respondents reported symptoms consistent with major depression; 23% of high school A and 15% of college A respondents had symptoms consistent with PTSD. Rates for symptoms consistent with depression and PTSD from the survey were significantly higher in high school A and college A compared with high school B and college B (Table 2). Reported by: BP Bernard, MD, SL Baron, MD, CA Mueller, MS, RJ Driscoll, PhD, LC Tapp, MD, KM Wallingford, MS, AL Tepper, PhD, National Institute for Occupational Safety and Health, CDC. Editorial Note:The findings from these surveys indicate that 4--6 months after the September 11 terrorist attacks, workers surveyed near the WTC site had substantial rates of irritative, respiratory, and mental health symptoms and lost work time, compared with similar workers surveyed >5 miles from the WTC site. These findings indicate how the impact of the WTC attacks extended beyond the WTC site to affect the health of persons working nearby. Mucous membrane and respiratory symptoms among the survey participants described in this report, the majority of whom were present during the September 11 attacks, might have resulted initially from exposure to multiple environmental contaminants (e.g., smoke, respirable airborne particles, fine dust, and fire combustion products) generated by the collapse of the towers and ensuing fires. Information is limited concerning health effects associated with complex mixed environmental exposures (e.g., those that occurred during and after the WTC attacks). Approximately 30% of workers included in this survey reported persistent physical symptoms several months after the initial event. The persistence of symptoms in certain persons might be explained by several factors, including differences in the initial exposure, individual susceptibility, existing medical conditions, and factors related to social support or individual stressors. The results reported here indicate that many high school and college workers near the WTC site experienced symptoms consistent with PTSD and depression. Proximity to the WTC site also was a significant finding for "probable PTSD" (a slightly different case definition using the same PTSD scale) among NYC residents in a recent web-based epidemiologic study (4). The findings in this report are subject to at least two limitations. First, responses to extraordinary traumatic events might provoke a range of reactions, and symptoms alone are not adequate to document fully psychologic or physical illness. Second, because of the low response rate for colleges A and B, the percentages and prevalence ratios should be interpreted with caution because of potential participation bias. Further investigations using full clinical diagnostic assessment might be useful in determining the breadth and scope of illness in persons with persistent symptoms. Because mental health and physical symptoms can persist for extended periods after a disaster, persons who continue to experience symptoms should seek professional assistance. Counseling services should continue to target those who are vulnerable to depression and PTSD, particularly those who have lost family or friends, those who do not have a social network, and those who witnessed the attacks (5,6). References
Table 1 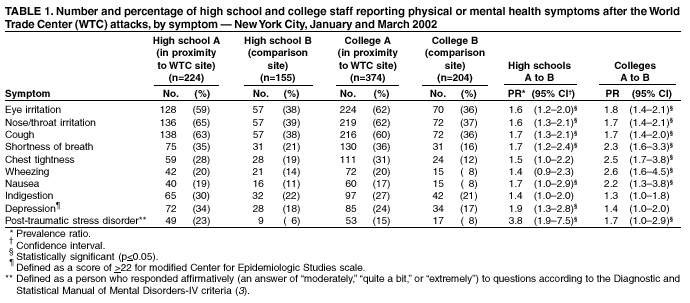 Return to top. Table 2 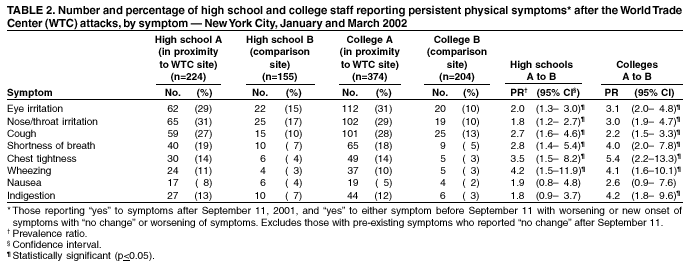 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/9/2002 |
|||||||||
This page last reviewed 9/9/2002
|