|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Increases in Fluoroquinolone-Resistant Neisseria gonorrhoeae --- Hawaii and California, 2001
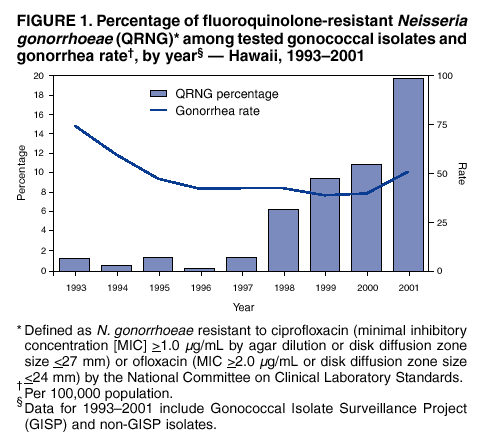
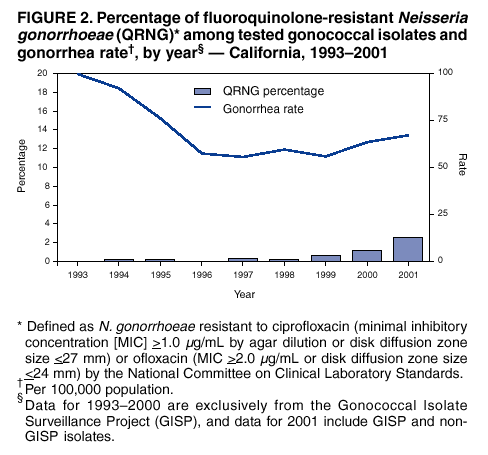
Neisseria gonorrhoeae is a major cause of pelvic inflammatory disease, ectopic pregnancy, and infertility, and it can facilitate human immunodeficiency virus (HIV) transmission (1). Gonorrhea is the second most frequently reported communicable disease in the United States, with 361,705 reported cases in 2001 (2). During the 1980s, gonococcal resistance to penicillin and tetracycline became widespread; as a result, CDC recommended using cephalosporins as first-line treatment for gonorrhea. Since 1993, CDC also has recommended using fluoroquinolones (i.e., ciprofloxacin, ofloxacin, or levofloxacin) for gonorrhea treatment. Fluoroquinolone therapy is used widely because it is a relatively inexpensive, oral, and single-dose therapy. However, fluoroquinolone-resistant N. gonorrhoeae (QRNG)* is being identified more frequently (3). This report summarizes investigations of increases in QRNG in Hawaii and California in 2001 and provides data to support the recommendation that cephalosporins (i.e., ceftriaxone or cefixime) be used instead of fluoroquinolones as first-line treatment for gonorrhea acquired in these two states. The increases in QRNG highlight the importance of monitoring gonococcal resistance throughout the United States to guide local treatment decisions. HawaiiIn 2001, the Hawaii State Laboratory performed gonorrhea culture and antimicrobial susceptibility tests on specimens from 265 (44%) of 605 reported gonorrhea cases. Patients seeking care at the public sexually transmitted disease (STD) clinic accounted for 44% (117 of 265) of these isolates. Overall, QRNG accounted for 20% (53 of 265) of gonococcal isolates tested, compared with 11% in 2000 and 10% in 1999 (Figure 1). In 2001, 36% (19 of 53) of QRNG infections were among STD clinic patients. Medical and interview records of the 117 STD clinic patients with positive gonococcal cultures diagnosed during January--December 2001 were reviewed to identify risk factors for QRNG; 19 (16%) had QRNG isolates. QRNG prevalence was higher for men who had sex exclusively with women than for men who had sex with men (MSM) (11 [20%] of 55 versus one [3%] of 29; p=0.05). Persons with a history of recent travel to Asia or a sex partner with such a history were not significantly more likely to have QRNG (four [36%] of 11) than persons without such a history (14 [14%] of 102; p=0.07). Unlike in Hawaii in 1999 (4), QRNG prevalence was not significantly higher among Asians/Pacific Islanders than among non-Asians/Pacific Islanders (10 [19%] of 54 versus nine [14%] of 63; p=0.54). Since 2000, the Hawaii Department of Health (HDH) has recommended that clinicians avoid using fluoroquinolones to treat gonorrhea. Because of the 25% increase in reported gonorrhea morbidity (from 39.9 cases per 100,000 population in 2000 to 49.9 in 2001), adherence to this recommendation is particularly important. In February 2002, HDH informed all clinicians of the increases in gonorrhea and QRNG and organized STD training for an expanded network of clinicians and workers in community-based organizations. Preliminary analysis of gonococcal susceptibility results for 147 patients during January--June 2002 suggests that QRNG prevalence remains >14%. CaliforniaSan Francisco, Long Beach, Orange County, and San Diego are participants in the Gonococcal Isolate Surveillance Project (GISP), a CDC-sponsored sentinel surveillance system that monitors antimicrobial resistance in N. gonorrhoeae through antimicrobial susceptibility testing of male urethral gonococcal isolates obtained from patients at public STD clinics in 26 U.S. cities. During 1990--2000, <1% of isolates tested annually from each GISP site in California were QRNG, except for Orange County, where 5.6% (six of 107) of GISP isolates were QRNG in 2000. In 2001, susceptibility testing was expanded beyond the GISP sample to include all gonococcal isolates from Orange County and San Diego STD clinic patients, including those from women and nonurethral sites. Susceptibility testing also was performed on all gonococcal isolates obtained from patients at a large southern California health maintenance organization (HMO) during February--April 2001. In 2001, QRNG was identified in 2.5% (33 of 1,311) of patients with tested isolates (Figure 2). Among STD clinic patients with gonorrhea, 3.4% (10 of 297) in San Francisco, 3.0% (three of 99) in Long Beach, 3.3% (seven of 212) in Orange County, and 2.4% (eight of 330) in San Diego had QRNG. Among HMO patients with gonorrhea, 1.3% (five of 373) had QRNG. The 1,311 patients with tested isolates accounted for 5.6% of all reported gonorrhea cases in California in 2001. Among 29 men infected with QRNG in 2001 whose sexual orientation was known, 20 (69%) were MSM. Among MSM with QRNG, 19 had a median of three recent (within 2--6 months) sex partners (range: one--40); 10 heterosexual men and women with QRNG had a median of 1.5 recent sex partners (range: one--eight), indicating the potential for more rapid spread among MSM. Although 12 (43%) of 28 QRNG patients interviewed in 2001 reported recent travel to Asia, the Pacific Islands, or Hawaii by themselves or a sex partner, 57% denied such travel, suggesting endemic spread of QRNG within California. Medical records were reviewed for all 469 gonorrhea patients whose isolates were tested for susceptibility and who were seen in San Francisco, Long Beach, Orange County, or San Diego STD clinics during July 1--December 31, 2001. QRNG was identified in 23 (4.9%) of the 469 patients tested. QRNG was more common among Asians/Pacific Islanders than among non-Asians/Pacific Islanders (four [16.7%] of 24 versus 19 [4.4%] of 427; p=0.03). QRNG prevalence was similar among MSM (5.2% [15 of 289]), heterosexual men (4.7% [seven of 149]), and women (3.6% [one of 28]). However, geographic variation was noted in California: in San Diego, QRNG was more common among MSM than among heterosexual men and women (6.6% [seven of 106] versus zero of 65; p=0.03), and in San Francisco, QRNG was more common among heterosexuals than among MSM (11.4% [five of 44] versus 1.1% [one of 93]; p=0.01). In response to the increasing prevalence of QRNG, in May 2002 the California Department of Health Services advised clinicians to avoid using fluoroquinolones for treatment of gonorrhea. Preliminary data collected during January--June 2002 indicate that the prevalence of QRNG infection among STD clinic patients with tested gonococcal isolates in GISP sites in California has increased, exceeding 9% during this period. Reported by: PM Whiticar, RG Ohye, MS, MV Lee, MS, Hawaii State Dept of Health. HM Bauer, MD, G Bolan, MD, STD Control Br, California Dept of Health Svcs. SA Wang, MD, RA Gunn, MD, HS Weinstock, MD, SM Berman, MD, Div of STD Prevention, National Center for HIV, STD, and TB Prevention; KE Mark, MD, LM Newman, MD, EIS officers, CDC. Editorial Note:These data demonstrate that in 2001, QRNG prevalence increased in Hawaii and in California, where the epidemiology of QRNG varies within the state. In California, antimicrobial susceptibility data are available for a smaller proportion of reported gonorrhea cases than in Hawaii (6% versus 44%). Demographic data suggest that this low proportion might limit the generalizability of California's findings: patients with susceptibility-tested isolates in California were more likely to be male, older, and white, and to have their condition diagnosed in STD clinics than were other gonorrhea patients. However, the data from California indicate that QRNG has reached the continental United States, increasing the risk for its spread. Sporadic cases of QRNG have been identified in other states through GISP and non-GISP reporting, but no sustained increase in QRNG >1% has been identified in any other state (3). Increases in QRNG in California and Hawaii highlight the ongoing need for monitoring antimicrobial susceptibilities of gonococcal isolates throughout the United States. CDC recommends that fluoroquinolones not be used to treat gonococcal infections acquired in Asia, where QRNG prevalence exceeds 40% (5); in the Pacific Islands, including Hawaii; in California; and in other areas with increased prevalence of fluoroquinolone resistance (6). The recommended treatment options for persons who might have acquired infection in those areas are cefixime (7), ceftriaxone, or spectinomycin. To select appropriate gonorrhea treatment in areas outside Hawaii and California, clinicians should ask suspected gonorrhea patients about their recent travel history and that of their sex partners (8). Treatment of gonorrhea with fluoroquinolones can continue in areas where the prevalence of resistance is <1% (9). In areas where resistance is >1%, health departments making local treatment recommendations for gonorrhea also should consider other local factors such as the overall prevalence of gonorrhea, the availability of antimicrobial susceptibility data, and the cost of various diagnostic and treatment options (10). Fluoroquinolones remain an important gonorrhea treatment option in the United States because they are inexpensive and easy to administer. In addition, their use might decrease use of cephalosporins and delay the development of cephalosporin resistance. As part of effective gonorrhea control, state health departments should monitor local gonococcal antimicrobial susceptibility prevalence routinely to assist in developing local treatment recommendations. Symptomatic treatment failures are not a reliable indicator of emerging antimicrobial resistance because gonococcal infections, especially in women, are frequently asymptomatic. In 2001, a survey of STD project areas found that nonculture gonococcal tests were used widely and that approximately half of project areas had antimicrobial susceptibility data (3). Because nonculture tests cannot provide antimicrobial susceptibility results, local gonococcal culture capacity should be maintained. The antimicrobial susceptibility testing panel should, at a minimum, include a fluoroquinolone, cefixime, ceftriaxone, spectinomycin, azithromycin, and any other drugs in local use for gonorrhea treatment. In cases of persistent gonococcal infection after treatment, clinicians should consider performing culture and antimicrobial susceptibility testing. In areas where fluoroquinolones are used for treating gonorrhea and small numbers of patients with QRNG are identified, health departments should notify and treat partners of patients with known QRNG to minimize the spread of resistance. Through their state and local health departments, clinicians and laboratorians should report treatment failures or resistant gonococcal isolates to CDC, telephone 404-639-8373; isolates may be submitted to CDC's Neisseria Reference Laboratory for confirmation testing, telephone 404-639-3470. Acknowledgments This report is based in part on assistance and data contributed by AM Vannier, MD, Southern California Kaiser Permanente Regional Reference Laboratories, Los Angeles, California. N O'Connor, Hawaii State Public Health Laboratory, Pearl City; P Effler, MD, Hawaii State Dept of Health. N DeAugustine, H Calvet, MD, M Lachica, City of Long Beach Dept of Health and Human Svcs, Long Beach; PR Kerndt, MD, Los Angeles County Dept of Health Svcs, Los Angeles; P Weismuller, DrPH, County of Orange Health Care Agency, Santa Ana; D Moore, PhD, P Hannah, Orange County Public Health Laboratory, Santa Ana; C Peter, PhD, D Kiefler, G Washabaugh, MPH, San Diego County Health and Human Svcs Agency, San Diego; JD Klausner, MD, L Fischer, MPA, V Zapitz, S Liska, DrPH, San Francisco Dept of Public Health, San Francisco; S Coulter, E Lopez, STD Control Br, California Dept of Health Svcs. F Judson, MD, Denver Gonococcal Isolate Surveillance Project (GISP) Regional Laboratory, Denver Health, Colorado. KK Holmes, MD, J Hale, MS, W Whittington, PhD, K Winterscheid, MS, Seattle GISP Regional Laboratory, Univ of Washington, Seattle. JS Knapp, PhD, DL Trees, PhD, Div of AIDS, STD, and TB Laboratory Research, National Center for Infectious Diseases; AB Harvey, SM Conner, MPH, Div of STD Prevention, National Center for HIV, STD, and TB Prevention, CDC. References
* Defined as N. gonorrhoeae resistant to ciprofloxacin (minimal inhibitory concentration [MIC] >1.0 µg/mL by agar dilution or disk diffusion zone size <27 mm) or ofloxacin (MIC >2.0 µg/mL or disk diffusion zone size <24 mm) by the National Committee on Clinical Laboratory Standards.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/21/2002 |
|||||||||
This page last reviewed 11/21/2002
|