 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
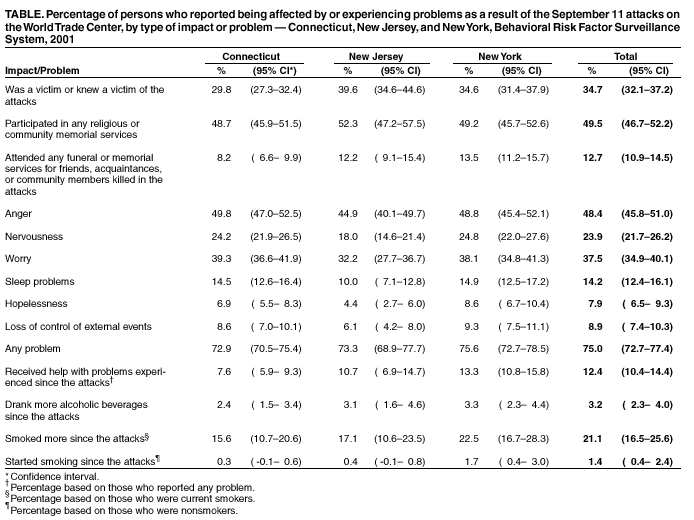
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Psychological and Emotional Effects of the September 11 Attacks on the World Trade Center --- Connecticut, New Jersey, and New York, 2001To measure the psychological and emotional effects of the September 11, 2001, terrorist attacks on the World Trade Center (WTC), Connecticut, New Jersey, and New York added a terrorism module to their ongoing Behavioral Risk Factor Surveillance System (BRFSS). This report summarizes the results of the survey, which suggest widespread psychological and emotional effects in all segments of the three states' populations. The findings underscore the importance of collaboration among public health professionals to address the physical and emotional needs of persons affected by the September 11 attacks. BRFSS is a random-digit--dialed telephone survey of the noninstitutionalized U.S. population aged >18 years (1,2). The terrorism module consisted of 17 questions which asked respondents whether they were victims of the terrorist attacks, attended a memorial or funeral service after the attacks, were employed or missed work after the attacks, increased their consumption of tobacco and/or alcohol following the attacks, or watched more media coverage following the attacks. The survey was conducted during October 11--December 31. A total of 3,512 respondents completed the module in the three states (1,774 in Connecticut, 638 in New Jersey, and 1,100 in New York). SAS and SUDAAN were used in the analyses to account for the complex sampling design. Of the 3,512 participants, approximately 50% participated in religious or community memorial services, and 13% attended a funeral or a memorial service for an acquaintance, relative, or community member (Table). Three fourths (75%) of respondents reported having problems attributed to the attacks. Nearly half (48%) of respondents reported that they experienced anger after the attacks. Approximately 12% of respondents with problems reported getting help. Family members (36%) and friends or neighbors (31%) were the main source for help. Approximately 3% of alcohol drinkers reported increased alcohol consumption, 21% of smokers reported an increase in smoking, and 1% of nonsmokers reported that they started to smoke after the attacks. The impact of the attacks varied by sex, age group, educational level, and race/ethnicity. Compared with men, women were more likely to have participated in a religious or community memorial service (55.1% [95% confidence interval (CI)=54.2%--55.9%] versus 43.0% [95% CI=41.7%--44.3%]) and to get help with the problems they experienced (15.3% [95% CI=13.0%--17.6%] versus 8.8% [95% CI=7.9%--9.6%]). Men were more likely than women to drink more alcohol (4.2% [95% CI=3.4%--4.9%] versus 2.4% [95% CI=2.1%--2.6%]), and women smokers were more likely than men to smoke more as a result of the attacks (27.1% [95% CI=23.9%--30.3%] versus 14.8% [95% CI=12.3%--17.3%]). Approximately 27% of respondents who were working at the time of the attacks missed work afterwards. The major reason for missing work was transportation problem (51%). Approximately 21% of workers had to be evacuated on the day of the attacks. Approximately 80% of respondents reported watching more media coverage than usual on television or through the Internet. Approximately 3% of respondents reported that they were victims of the attacks, 7% had relatives who were victims, and 14% had friends who were victims. In Connecticut, New Jersey, and New York, 4%, 17%, and 35% of the respondents, respectively, reported being in New York City during the attacks. Reported by: TA Melnik, DrPH, CT Baker, Bur of Chronic Disease Epidemiology and Surveillance, New York State Dept of Health. ML Adams, MPH, Connecticut Dept of Health. K O'Dowd, PhD, New Jersey Dept of Health and Senior Svcs. AH Mokdad, PhD, DW Brown, MSPH, W Murphy, WH Giles, MD, VS Bales, MPH, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report document the widespread emotional and psychological effects among residents of three states following the September 11 attacks and indicate that some persons sought help to cope with the catastrophic events. Although this survey inquired about the short-term effects of the attacks, the findings suggest the need to consider the long-term emotional and psychological health of the affected population. The flexible design of BRFSS allows states to add questions to their ongoing surveys to address changing situations and crises, such as the WTC attacks. The findings in this report are subject to at least four limitations. First, the survey design excluded persons without a telephone, which primarily includes persons of low socioeconomic status. Second, the survey excluded persons who were not yet able to discuss their emotional response to the attacks. Third, the survey did not measure the severity and duration of emotional and psychological problems of the respondents. Finally, the survey might have excluded persons who had moved from the area after the attacks. Public health professionals should consider the emotional and psychological well-being of persons after traumatic events. The results of community-based surveys can help target programs designed to help residents deal with the aftermath of terrorist attacks. In response to national disasters, several programs have been implemented successfully to provide immediate medical care and to prevent the spread of infections and disease; however, the long-term emotional pain and suffering associated with disasters also needs to be considered in response planning. State and federal agencies should prepare programs to address the emotional and psychological health of persons, and these programs should be integrated with other disaster-preparedness plans. References
 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/5/2002 |
|||||||||
This page last reviewed 9/5/2002
|