|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
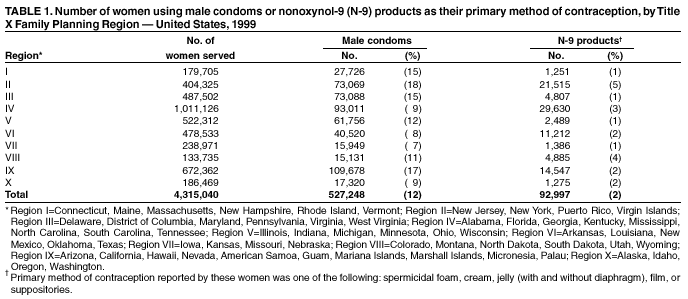
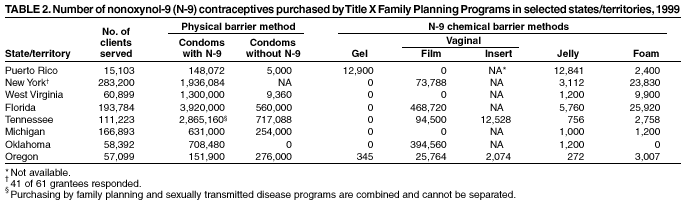
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Nonoxynol-9 Spermicide Contraception Use --- United States, 1999Most women in the United States with human immunodeficiency virus (HIV) become infected through sexual transmission, and a woman's choice of contraception can affect her risk for HIV transmission during sexual contact with an infected partner. Most contraceptives do not protect against transmission of HIV and other sexually transmitted diseases (STDs) (1), and the use of some contraceptives containing nonoxynol-9 (N-9) might increase the risk for HIV sexual transmission. Three randomized, controlled trials of the use of N-9 contraceptives by commercial sex workers (CSWs) in Africa failed to demonstrate any protection against HIV infection (2--4); one trial showed an increased risk (3). N-9 contraceptives also failed to protect against infection with Neisseria gonorrhoeae and Chlamydia trachomatis in two randomized trials (5,6), one among African CSWs and one among U.S. women recruited from an STD clinic. Because most women in the African studies had frequent sexual activity, had high-level exposure to N-9, and probably were exposed to a population of men with a high prevalence of HIV/STDs, the implications of these studies for U.S. women are uncertain. To determine the extent of N-9 contraceptive use among U.S. women, CDC assessed data provided by U.S. family planning clinics for 1999. This report summarizes the results of that assessment, which indicate that some U.S. women are using N-9 contraceptives. Sexually active women should consider their individual HIV/STD infection risk when choosing a method of contraception. Providers of family planning services should inform women at risk for HIV/STDs that N-9 contraceptives do not protect against these infections. CDC collected information on types of N-9 contraceptives purchased and family planning program (FPP) guidelines for N-9 contraceptive use. The national FPP, authorized by Title X of the Public Health Service Act, serves approximately 4.5 million predominantly low-income women each year. Program data for 1999 were obtained from all 10 U.S. Department of Health and Human Services (HHS) regions on the number of female clients and the number of female clients who reported use of N-9 contraceptives or condoms as their primary method of contraception. CDC obtained limited purchase data for 1999 for specific N-9 contraceptives and program guidelines from eight state/territorial FPPs within six HHS regions. State health departments, family planning grantees, and family planning councils were contacted to request assistance in collecting data on purchasing patterns of the 91 Title X grantees; of the 12 FPPs that responded, eight provided sufficient data for analysis. In 1999, a total of 7%--18% of women attending Title X clinics reported using condoms as their primary method of contraception. Data on the percentage of condoms lubricated with N-9 were not available. A total of 1%--5% of all women attending Title X clinics reported using N-9 contraceptives (other than condoms) as their primary method of contraception (Table 1). Among the eight FPPs that provided purchase data, most (87%) condoms were N-9--lubricated (Table 2). All eight FPPs purchased N-9 contraceptives (i.e., vaginal films and suppositories, jellies, creams, and foams) to be used either alone or in combination with diaphragms or other contraceptive products. Four of the eight clinics had protocols or program guidance stating that N-9--containing foam should be dispensed routinely with condoms; two additional programs reported that despite the absence of a clinic protocol, the practice was common. Data for the other two programs were not available. Reported by: The Alan Guttmacher Institute, New York, New York. Office of Population Affairs, U.S. Dept of Health and Human Services, Bethesda, Maryland. A Duerr, MD, C Beck-Sague, MD, Div Reproductive Health, National Center Chronic Disease and Public Health Promotion; Div of HIV and AIDS Prevention, National Center HIV/AIDS, STDs, and TB Prevention; B Carlton-Tohill, EIS Officer, CDC. Editorial Note:The findings in this report indicate that in 1999, before the release of recent publications on N-9 and HIV/STDs (4,6,7), Title X family planning clinics in the U.S. purchased and distributed N-9 contraceptives. Among at least eight family planning clinics, most of the condoms purchased were N-9--lubricated; this is consistent with trends in condom purchases among the general public (8). The 2002 STD treatment guidelines state that condoms lubricated with spermicides are no more effective than other lubricated condoms in protecting against the transmission of HIV infection and other STDs (7). CDC recommends that previously purchased condoms lubricated with N-9 spermicide continue to be distributed provided the condoms have not passed their expiration date. The amount of N-9 on a spermicide-lubricated condom is small relative to the doses tested in the studies in Africa and the use of N-9--lubricated condoms is preferable to using no condom at all. In the future, purchase of condoms lubricated with N-9 is not recommended because of their increased cost, shorter shelf life, association with urinary tract infections in young women, and lack of apparent benefit compared with other lubricated condoms (7). Spermicidal gel is used in conjunction with diaphragms (1); only diaphragms combined with the use of spermicide are approved as contraceptives. The respective contributions of the physical barrier (diaphragm) and chemical barrier (spermicide) are unknown, but the combined use prevents approximately 460,000 pregnancies in the United States each year (1). The findings in this report are subject to at least two limitations. First, data on specific products and patterns of contraceptive use were limited; CDC used a nonrepresentative sample of regions and states that voluntarily provided data, and specific use patterns of the contraceptives could not be extrapolated from these data. Second, data correlating use of N-9 contraceptives with individual HIV risk were not available. Prevention of both unintended pregnancy and HIV/STD infection among U.S. women is needed. In 1994, a total of 49% of all pregnancies were unintended (9). Furthermore, 26% of women experience an unintended pregnancy during the first year of typical use of spermicide products (1). In 1999, a total of 10,780 AIDS cases, 537,003 chlamydia cases, and 179,534 gonorrhea cases were reported among U.S. women. Contraceptive options should provide both effective fertility control and protection from HIV/STDs; however, the optimal choice is probably not the same for every woman. N-9 alone is not an effective means to prevent infection with HIV or cervical gonorrhea and chlamydia (2,7). Sexually active women and their health-care providers should consider risk for infection with HIV and other STDs and risk for unintended pregnancy when considering contraceptive options. Providers of family planning services should inform women at risk for HIV/STDs that N-9 contraceptives do not protect against these infections. In addition, women seeking a family planning method should be informed that latex condoms, when used consistently and correctly, are effective in preventing transmission of HIV and can reduce the risk for other STDs. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/9/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 5/9/2002