|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
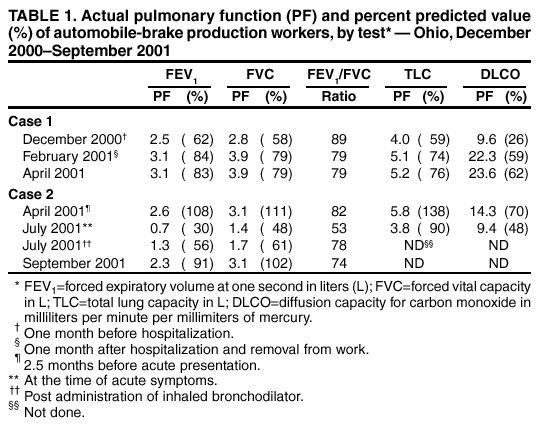
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Respiratory Illness in Workers Exposed to Metalworking Fluid Contaminated with Nontuberculous Mycobacteria --- Ohio, 2001In January 2001, three machinists at an automobile brake manufacturing facility in Ohio (plant A) were hospitalized with respiratory illness characterized by dyspnea, cough, fatigue, weight loss, hypoxia, and pulmonary infiltrates. Hypersensitivity pneumonitis (HP) was diagnosed in all three workers. In March 2001, additional employees began seeking medical attention for respiratory and systemic symptoms. In May 2001, union and management representatives requested assistance from CDC's National Institute for Occupational Safety and Health (NIOSH) in determining the cause of the illnesses and preventing further illness in employees. This report describes two case reports and the preliminary results of the ongoing investigation, which found that exposure to aerosolized nontuberculous mycobacteria (NTM) might be contributing to the observed respiratory illnesses in this manufacturing facility. Clinicians and public health professionals should be alert to the variable presentation of occupational respiratory disease that might occur in workers in the machining industry. Plant A is an automobile brake manufacturing facility machining primarily cast-iron parts. Approximately 400 persons work at plant A, including approximately 150 workers in machining areas and 250 workers in nonmachining areas. The nonmachining areas of plant A are separated from the machining areas by a wall and are serviced by a separate ventilation system. Plant A machines receive metalworking fluid (MWF) from either dedicated sumps or one of four central MWF systems, with volumes of 4,500--20,000 gallons. The semisynthetic MWF in use at the plant included a formaldehyde-releasing biocide; a second biocide (isothiazolinone-based) was added as indicated to control microbial growth. Case ReportsCase 1. In mid-January 2001, a male machinist aged 45 years who had been employed at plant A for 26 years was hospitalized for worsening respiratory symptoms, hypoxia, and pulmonary infiltrates. He had been treated by his family physician 1 month earlier with a course of antibiotics for a nonspecific respiratory illness that improved during a holiday layoff from work. On his return to work in early January 2001, the patient's symptoms of dyspnea, chest tightness, and non-productive cough recurred. On admission, a high-resolution computed tomography (HRCT) scan revealed diffuse interstitial infiltrates with a nodular pattern superimposed on the infiltrates. Oxygen tension on room air at rest was 49 millimeters of mercury (mm Hg) (normal: 80--100 mm Hg) with 87% saturation (normal: 96%--100%); a white blood cell count was 8,000 (normal: 4,800--10,800) with a normal differential; and a Legionella titer was <1:256 (normal: <1:256). HP was diagnosed, and the patient was removed from work and treated with intravenous, oral, and inhaled corticosteroids and with bronchodilators. Repeat HRCT scan 1 month after hospitalization, while the patient was still away from work, revealed clear lung fields. Pulmonary function tests (PFTs) revealed improvement in initial restrictive findings and diffusing capacity (Table 1). Two months after hospitalization, oxygen saturation on room air at rest was 96%. Serum precipitin analysis was strongly positive for precipitating antibodies to Mycobacterium sp. cultured in February 2001 from MWF at plant A (1). The same tests performed on two co-workers from plant A who also had been hospitalized in January 2001 with HP also were strongly positive. Case 2. In July 2001, a woman aged 47 years presented to a private physician with a 1-day history of dyspnea, cough, chest tightness, wheezing, epistaxis, nausea, emesis, and fatigue that began <2 hours after she began steam-cleaning machining equipment in plant A. She had not performed this type of job previously and wore no respiratory protection. Physical examination revealed diminished breath sounds in all lung fields. Oxygen tension was 65 mm Hg with 92% saturation. PFTs revealed an obstructive deficit that improved after the administration of bronchodilators (Table 1). HRCT was normal. Occupational asthma and hypoxemia were diagnosed; the patient was removed from work and treated with oral and inhaled corticosteroids and with bronchodilators. The patient returned to work in August 2001; follow-up PFTs (Table 1) and oxygen saturation were within normal ranges. Medical Record ReviewIn November 2001, CDC investigators reviewed plant A records and found that 107 (27%) of 400 workers had been placed on work restriction by their treating physicians during the preceding 11 months because of respiratory conditions; 37 (35%) of these 107 workers remained on medical leave and 70 (65%) had returned to work. Medical records through October 2001 were reviewed for 32 (86%) of the 37 workers remaining on medical leave. All 32 workers had either full- or part-time work duties in the machining side of the plant; the median length of time working at plant A was 18 years (range: 3--32 years). Initial symptom onset for these workers occurred during October 2000--April 2001, with onset for 13 of these 32 workers occurring in December 2000. Of the 32 workers, 14 (44%) met a definition for occupational asthma (OA)* and 12 (38%) met a definition for HP†. Of the six workers with respiratory or upper respiratory symptoms not meeting definitions for OA or HP, three had illnesses consistent with work-related bronchitis, two had illnesses consistent with work-related rhinosinusitis, and one was symptomatic primarily with dyspnea. Environmental SamplingMultiple samples of bulk MWF from all central MWF systems at plant A analyzed for microbial contaminants during February--July 2001 revealed predominant growth of M. immunogenum, a newly proposed species of the Mycobacterium abscessus/Mycobacterium chelonae group (2), at levels up to 106 colony-forming units per milliliter. Subsequent sampling conducted weekly since July 2001 has revealed noncultivable mycobacteria at decreasing concentrations§ but virtually no viable bacteria. Area and personal air sampling performed during April 2001 in the machining areas revealed concentrations of MWF aerosol of <0.1--0.9 milligrams of total particulate per cubic meter (mg/m3) of air (median: 0.6 mg/m3). Two of five personal samples were above the NIOSH-recommended exposure limit (REL).¶ To minimize potential exposures to MWF and MWF contaminants, plant A conducted steam-cleaning of the MWF systems and machines, improved local ventilation of selected machines, and installed a conditioned air system for the machining areas and fresh MWF combined with a new biocide effective against mycobacteria. No workers at plant A with symptom onset after April 2001 have been identified. Local health-care providers continue to monitor workers who have been ill and assess their ability to return to work. Plant A and CDC representatives are assessing control measures already in place and the need for additional measures. Reported by: L Weiss, MD, Knox Community Hospital, Mount Vernon; C Pue, MD, Central Ohio Pulmonary Disease, Columbus; R Lewis, MD, Cleveland, Ohio. H Rossmoore, PhD, Biosan Laboratories, Warren, Michigan. J Fink, MD, Milwaukee, Wisconsin. J Harney, MS, D Trout, MD, Div of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health, CDC. Editorial Note:This report, combined with previously published data, suggests that exposure to aerosolized NTM might be contributing to the observed respiratory illnesses in this manufacturing facility. Illnesses reported in persons with exposure to aerosolized NTM have included HP (3,4) and other pulmonary diseases difficult to classify as hypersensitivity or true infection (5,6). However, because pulmonary illness in machinists has been described in outbreaks in which NTM have not been implicated as a primary contaminant (1) and NTM have been cultured from MWF in plants without reported respiratory illness (CDC, unpublished data, 2001), the importance of finding any specific microbe as an MWF contaminant remains uncertain. The spectrum of illnesses observed in machinists in this outbreak indicates that several mechanisms of illness probably are occurring. HP is a diffuse interstitial granulomatous lung disease involving an immunologic reaction of the lung to repeated inhalation of foreign antigens. OA is a disease of the airways that can be caused by immunologic and irritant reactions. The known irritant effects of MWF and MWF contaminants might be contributing to observed health effects; however, because affected employees generally have worked for many years in the machining environment without reported problems before the outbreak, other factors also are probably contributing to illness. The ability to determine specific exposure at plant A related to respiratory illnesses is limited for at least three reasons. First, the specific agent(s) causing these illnesses remains undetermined, and clinical and/or laboratory tests are needed to identify specific constituents or contaminants of MWF related to observed respiratory illness. Second, actual personal exposures to MWF, contaminants in MWF, or other substances in the work environment remain unknown for most workers who have become ill. Finally, illness might be misclassified because affected workers presented most commonly with signs and symptoms that appeared to represent a mixture of interstitial, airway, and upper respiratory effects not easily classifiable into well-established categories of occupational illness (e.g., HP or OA). The findings in this report represent one of the largest reported outbreaks of work-related respiratory illness in the machining environment in the United States and have health implications for the estimated one million workers occupationally exposed to MWF (1,4,7). Because the etiologic agents responsible for the observed illnesses are unknown, employees, unions, manufacturing companies involved in machining processes and private and public health professionals must be educated about appropriate prevention and control measures, including appropriate engineering controls, MWF management practices, and use of personal protective equipment (8--10). Early recognition of potential occupational illness in workers in the machining environment and ongoing medical surveillance for these workers also are needed to detect and prevent both acute illness and irreversible respiratory impairment. References
* Defined as one or more work-related respiratory symptoms (cough, dyspnea, wheezing, or chest tightness) and the absence of systemic signs or symptoms; no infiltrate seen on CXR or HRCT scan; and spirometry consistent with reversible airway obstruction (an obstructive pattern with >12% improvement in FEV1 after administration of inhaled bronchodilators). † Defined as the presence of one or more work-related respiratory symptoms (cough, dyspnea, wheezing, or chest tightness), one or more systemic signs or symptoms (fever, chills, extreme fatigue, myalgia, or night sweats), an infiltrate seen on chest radiograph or HRCT scan, and abnormal spirometry (either an obstructive or restrictive pattern). § Assessed semi-quantitatively by comparison of microscopic evaluation (acid-fast stain) of a pellet obtained by centrifugation of an MWF sample (which evaluates both viable and nonviable organisms) with culture techniques (which evaluate viable organisms). ¶ REL for MWF aerosol=0.5 milligrams of total particulate (0.4 milligrams of thoracic particulate) per cubic meter of air.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 4/24/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 4/24/2002