 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Socioeconomic Status of Women with Diabetes --- United States, 2000Persons whose socioeconomic status is low have poorer health than other persons (1,2) and are less likely to have adequate access to care or to receive high-quality clinical and prevention care services (3). In the United States, diabetes is a potentially debilitating disease that is increasing in prevalence (4); however, little is known about the socioeconomic status of persons with diabetes (5--7). Women account for approximately 52% of all persons aged >20 years with diabetes (4). To assess the socioeconomic status of women with diabetes, CDC analyzed data from the Behavioral Risk Factor Surveillance System (BRFSS), which indicated that the socioeconomic status of women with diabetes in 2000 was markedly lower than that of women without diabetes. Efforts should be focused to understand the impact of socioeconomic conditions on the health and quality of care of women with diabetes. BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized U.S. population aged >18 years. In 2000, the median state-specific response rate was 48.9% (range: 28.8%--71.8%) (CDC, unpublished data, 2001). Persons with diabetes were identified if they answered "yes" to the question, "Have you ever been told by a doctor that you have diabetes?" Women who answered "no" and those who had been told they had diabetes only during pregnancy were considered not to have diabetes. Data on level of education and annual household income were used to assess socioeconomic status; marital status, size of household, and employment status were used as indicators of living arrangements; and household size was derived by adding the number of adults and number of children aged <17 years. A woman was classified as having low socioeconomic status if she did not complete high school or resided in a household with an annual income of <$25,000. State-specific data were aggregated and weighted to reflect age, sex, and racial/ethnic distribution, and chi-square tests were used to test all univariate associations. Because many persons aged 18--24 years have not completed their education, socioeconomic status was evaluated only for women aged >25 years. Multivariate logistic regression analysis was used to examine the relation between having diabetes and not completing high school or living in a low-income household, with control made for age, race/ethnicity, and living arrangements. The models then were used to calculate adjusted percentages using the distributions of female respondents aged >25 years in the total population. All analyses were conducted using SASv8 software with SUDAAN to estimate standard errors. Of the 109,680 women who participated in the 2000 BRFSS survey, 6,835 (6.3%) had been told by a doctor that they had diabetes (mean age at diagnosis: 48.8 years). Women with diabetes were more likely than women without diabetes to be aged >45 years; nonwhite; divorced, separated, or widowed; living alone; retired; or unable to work (Table 1). Among women aged >25 years, the percentage with diabetes who had not completed high school (27.7%; 95% confidence interval [CI]=25.7%--29.7%) was more than twice that of women without diabetes who had not completed high school (12.2%; 95% CI=11.8%--12.6%) (Table 2). Among women with diabetes, 20.5% (95% CI=18.0%--25.3%) of those aged 25--44 years had not completed high school, compared with 34.3% (95% CI=31.4%--37.2%) of those aged >65 years. Among women without diabetes, 9.8% (95% CI=9.2%--10.3%) of those aged 25--44 years had not completed high school, compared with 20.5% (95% CI=19.5%--21.5%) of those aged >65 years. After multivariate adjustment, a low level of formal education remained significantly more common among women with diabetes than among those without diabetes. Overall, women with diabetes (40.4% [95%CI=38.1%--42.6%]) were approximately twice as likely as women without diabetes (22% [95% CI=21.5%--22.5%]) to have an annual household income <$25,000. Among women with diabetes, the percentages with incomes <$25,000 were highest for women aged >65 years (47.8% [95% CI=44.4%--51.1%]) and those aged <44 years (41.3% [95% CI=35.4%--47.2%]) and lowest (33% [95% CI=29.5%--36.6%) for women aged 45--64 years (Table 2). In each age group, percentages were lower for women without diabetes (32.9%, 19.7%, and 18.6%, respectively). After multivariate adjustment, the difference between women with and without diabetes remained significant. Reported by: GLA Beckles, MD, PE Thompson-Reid, MPH, Div of Diabetes Translation, National Center for Chronic Disease and Health Promotion, CDC. Editorial Note:The findings in this report indicate that the socioeconomic status of women with diabetes is lower than that of women without diabetes and confirm the findings of the 1989 National Health Interview Survey (NHIS) (5). In 2000, at least one in four women with diabetes aged >25 years had a low level of formal education, and 40% lived in low-income households. Women with diabetes were more likely to have a low socioeconomic status independent of living arrangements (i.e., marital status, size of household, and employment status). Attaining a higher educational level might influence decision-making, and persons with a higher income might have better access to health care, higher living standards, and other material benefits that have a positive impact on health. Although socioeconomic status might be influenced adversely by factors related to having diabetes (e.g., being unemployed or retiring early), most women with diabetes in this survey were diagnosed long after they had completed their education. BRFSS estimates suggest that the low socio-economic status of many women with diabetes might compromise their ability to benefit from treatments that might reduce their risks for complications and premature death. Programs designed to meet the needs of women with diabetes should take socioeconomic status into account to assure that women benefit from the interventions. Performance should be carefully evaluated to assess program effectiveness and identify areas for improvement. The findings in this report are subject to at least three limitations. First, the low median response rate suggests the potential for participation bias. Second, all data were self-reported and might be subject to recall bias. Finally, the level of low socioeconomic status (i.e., household income <$25,000) among women with diabetes might be under-estimated because 21% of women with diabetes declined to state their income; these nonrespondents were more likely to be elderly, Hispanic, widowed, retired, or not to have completed high school (i.e., to belong to groups that are frequently low income). CDC has initiated activities that focus on the needs of women with diabetes. CDC's "Diabetes and Women's Health Across the Life Stages: A Public Health Perspective" analyzes the epidemiologic, social, and environmental dimensions of women and diabetes and discusses public health implications (8). CDC, the American Diabetes Association, the American Public Health Association, and the Association of State and Territorial Health Officials are developing a National Public Health Action Plan for Diabetes and Women. CDC is sponsoring Translating Research into Action for Diabetes (TRIAD), a 5-year prospective study of the quality of diabetes care, costs, and outcomes in managed-care settings that will examine the effects of socioeconomic status on health and quality of care. Finally, CDC is encouraging increased focus on women with diabetes through the National Diabetes Education Program, a collaborative effort with the National Institutes of Health to promote early diagnosis and improvement of the treatment and outcomes for persons with diabetes (available at http://www.cdc.gov/diabetes/projects/ndeps.htm); Racial and Ethnic Approaches to Community Health (REACH) 2010, a program aimed at eliminating disparities in the health status of ethnic minorities (available at http://www.cdc.gov/reach2010), and state-based diabetes control programs. The low socioeconomic status of many women with diabetes poses challenges to public health practitioners. As the prevalence of diabetes continues to increase, continued and creative efforts will be needed to gain greater understanding of how socioeconomic status affects the health of women with diabetes. Acknowledgement This report is based on data contributed by state BRFSS coordinators. References
Table 1 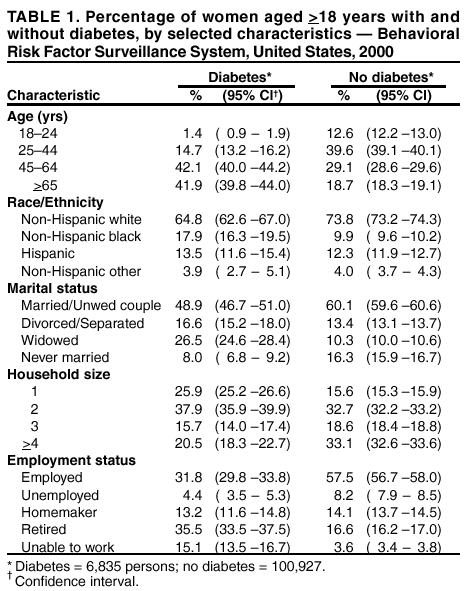 Return to top. Table 2 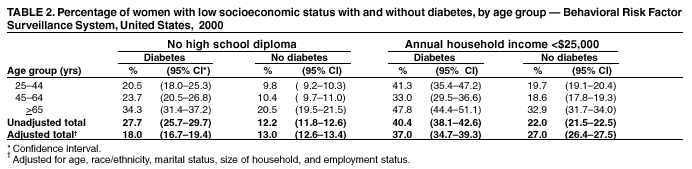 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 2/21/2002 |
|||||||||
This page last reviewed 2/21/2002
|