 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. State-Specific Prevalence of Current Cigarette Smoking Among Adults, and Policies and Attitudes About Secondhand Smoke ---United States, 2000Tobacco use, particularly cigarette smoking, is the leading preventable cause of death in the United States, but the health consequences extend beyond smokers to nonsmokers involuntarily exposed to environmental tobacco smoke or secondhand smoke (SHS) (1). Each year, an estimated 3,000 lung cancer deaths and 62,000 deaths from coronary heart disease in adult nonsmokers are attributed to SHS (2). Among children, SHS causes sudden infant death syndrome, low birthweight, chronic middle ear infections, and respiratory illnesses (e.g., asthma, bronchitis, and pneumonia) (2). Two national health objectives for 2010 are to reduce cigarette smoking among adults to 12% (objective 27-1) and the proportion of nonsmokers exposed to environmental tobacco smoke to 45% (objective 27-10) (1). To characterize state-specific prevalence of cigarette smoking among adults, exposure to SHS at home, smoke-free workplace policies, and attitudes toward smoke-free policies by state, CDC analyzed data from the 2000 Behavioral Risk Factor Surveillance System (BRFSS). This report summarizes the results of that analysis and indicates that in 2000, state-specific adult smoking prevalence ranged from 12.9%--30.5%, and high levels of public support exist, even among smokers, for smoke-free policies in many settings. States should implement comprehensive programs to reduce tobacco use and adopt clean indoor air policies to reduce involuntary exposure to SHS. BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized U.S. population aged >18 years. The 2000 BRFSS was conducted in the 50 states, the District of Columbia (DC), and Puerto Rico. To determine current cigarette smoking, respondents were asked, "Have you smoked at least 100 cigarettes in your entire life?" and "Do you now smoke cigarettes every day, some days, or not at all?" Current smokers were defined as those who reported having smoked >100 cigarettes during their lifetime and who currently smoked every day or some days. Respondents in 20 states were asked questions on smoking in the home, awareness of an official workplace smoke-free policy, and their attitudes about smoking bans in specific areas. To assess home exposure to SHS, respondents were asked, "In the past 30 days has anyone, including yourself, smoked cigarettes, cigars, or pipes anywhere inside your home?" Those who reported no smoking in the home during the preceding 30 days provided some indication of protection from exposure but not the existence of any rules or policies about smoking in the home. To assess awareness of workplace smoking policies, respondents who reported working indoors most of the time were asked, "Which of the following best describes your place of work's official smoking policy for indoor public or common areas, such as lobbies, rest rooms, and lunch rooms?" and "Which of the following best describes your place of work's official smoking policy for work areas?" Possible responses for both questions were "not allowed in any public/work areas," "allowed in some public/work areas," "allowed in all public/work areas," or "no official policy." To assess attitudes about smoke-free policies, respondents were asked, "In the following locations, do you think that smoking should be allowed in all areas, some areas, or not allowed at all?" These locations were restaurants, schools, day care centers, and indoor work areas. The percentage of respondents who reported that no smoking was allowed in the home, that smoking was not allowed in work areas, and that smoking should not be allowed at all in restaurants, schools, day care centers, and indoor work areas was calculated and reported by state. Estimates were weighted by age, race/ethnicity, and sex distribution of each state's population, and 95% confidence intervals were calculated using SUDAAN. Statistical significance was determined on the basis of nonoverlapping confidence intervals. The median response rate was 53.2% (range: 35.5%--77.7%). The cigarette smoking prevalence in 2000 differed approximately twofold (Table 1). The 12 areas with the highest prevalence of current smoking (Kentucky, Nevada, Missouri, Indiana, Ohio, West Virginia, North Carolina, Tennessee, New Hampshire, Alabama, Arkansas, and Alaska) differed significantly from the 12 areas with lower prevalence (Utah, Puerto Rico, California, Arizona, Montana, Hawaii, Minnesota, Connecticut, Massachusetts, Colorado, Maryland, and Washington). The median smoking prevalence among men was 24.4% (range: 14.5%--33.4%) and among women was 21.2% (range: 9.9%--29.5%). Utah had the lowest prevalence for men (14.5%) and Puerto Rico had the lowest for women (9.9%). For the 20 states that collected optional information, the proportion of adults reporting no smoking in their home during the 30 days preceding the survey ranged from 60.8% in West Virginia to 79.0% in Colorado (Table 2). The proportion of adults who work primarily indoors and reported an official workplace policy that no smoking was allowed in indoor public or common areas and work areas ranged from 61.4% in Mississippi to 83.9% in Montana. The proportion who thought that smoking should not be allowed in restaurants ranged from 44.3% in North Carolina to 63.6% in Montana. The proportion who thought that smoking should not be allowed at all in schools and day care centers was uniformly high. The proportion who thought that smoking should not be allowed at all in indoor work areas ranged from 66.4% in Wisconsin to 83.8% in DC. Current smokers and nonsmokers reported similar attitudes about not allowing smoking at all in schools (median: 89.1% for smokers and 95.6% for nonsmokers) and day care centers (median: 94.2% for smokers and 97.6% for nonsmokers); however, the proportion who thought smoking should not be allowed at all differed widely between smokers and nonsmokers for restaurants (median: 25.9% for smokers versus 66.2% for nonsmokers) and indoor work areas (median: 57.6% for smokers versus 82.1% for nonsmokers). Reported by the following BRFSS coordinators: S Reese, MPH, Alabama; P Owens, Alaska; R Weyant, Arizona; B Woodson, Arkansas; B Davis, PhD, California; D Brand, MSPH, Colorado; M Adams, MPH, Connecticut; F Breukelman, Delaware; J Davies-Cole, District of Columbia; S Oba, MSPH, Florida; L Martin, MS, Georgia; F Reyes-Salvail, MS, Hawaii; J Aydelotte, MA, Idaho; B Steiner, MS, Illinois; L Stemnock, Indiana; D Shepherd, PhD, Iowa; C Hunt, Kansas; T Sparks, Kentucky; B Bates, MSPH, Louisiana; J Graber, MS, Maine; H Lopez, Maryland; D Brooks, MPH, Massachusetts; H McGee, MPH, Michigan; N Salem, PhD, Minnesota; D Johnson, MS, Mississippi; J Jackson-Thompson, PhD, Missouri; P Feigley, PhD, Montana; L Andelt, PhD, Nebraska; E DeJan, MPH, Nevada; J Porter, New Hampshire; G Boeselager, MS, New Jersey; W Honey, MPH, New Mexico; C Baker, New York; Z Gizlice, PhD, North Carolina; L Shireley, MPH, North Dakota; P Pullen Coss, Ohio; K Baker, MPH, Oklahoma; K Pickle, MPH, Oregon; L Mann, Pennsylvania; Y Cintron, MPH, Puerto Rico; J Hesser, PhD, Rhode Island; M Wu, MD, South Carolina; M Gildemaster, South Dakota; D Ridings, Tennessee; K Condon, MS, Texas; K Marti, Utah; C Roe, MS, Vermont; J Hicks, PhD, Virginia; K Wynkoop Simmons, PhD, Washington; F King, West Virginia; K Pearson, Wisconsin; M Futa, MA, Wyoming. Cardiovascular Health Br, Div of Adult and Community Health; and Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The median prevalence of current smoking in 2000 was similar to that reported for the preceding 5 years. However, smoking prevalence varied among the states, DC, and Puerto Rico. The national health objective for 2000 of <15% of adults smoking cigarettes was achieved by Puerto Rico, Utah, and in California for women (objective 3.4) (3). The low prevalence in Utah and Puerto Rico may be a result of stronger social and cultural norms against tobacco use compared with other parts of the country. California's efforts to change social norms about smoking through large-scale social interventions have been temporally linked to a reduction in tobacco use (4). According to the Surgeon General, if the recommendations from the 2000 report Reducing Tobacco Use for a comprehensive program combining social, educational, clinical, economic, and regulatory strategies were implemented fully, the 2010 national health objectives related to tobacco use could be met (4). Similarly, decreases in adult prevalence in other states could be accelerated if the funding guidelines for comprehensive tobacco-control programs were followed more widely (5). The findings in this report are subject to at least four limitations. First, the prevalence estimates may be affected by a low response rate. Second, smoking data were based on self-reports without biochemical verification; however, self-reporting has generally been found to be accurate in population-based surveys among adults (6). Third, telephone surveys may result in both response and sampling bias because of greater nonresponse from subgroups at higher risk for smoking. Finally, respondents' definition of "official policy" may vary, and the validity of self-report of workplace policies is unknown. As of December 1999, 45 states and DC reported some restricted smoking in public places; however, many state and local laws for clean indoor air reduce but do not eliminate involuntary exposure to tobacco smoke (4). During 1988--1991 to 1999, exposure to SHS among nonsmokers aged >3 years decreased 75%; however, men, persons aged <20 years, and blacks continued to have substantially higher levels of exposure compared with those of women, persons aged >20 years, and other racial/ethnic groups (7). In addition, smoke-free workplace policies protected approximately 70% of the U.S. workforce in 1999, but protection levels varied widely among states (8). Involuntary exposure to SHS remains a common public health hazard that is preventable by appropriate regulatory policies (4). Bans on smoking in public places reduce exposure to SHS and the number of cigarettes smoked by smokers (9). The findings in this report indicate support for smoking bans, with nearly universal support for bans in schools and day care centers and strong support for bans in indoor work areas and restaurants. Clean indoor air policies are one way to change social norms about smoking and reduce tobacco consumption, but comprehensive approaches are needed to achieve the national health objectives for 2010 to reduce smoking prevalence and involuntary exposure to SHS. References
Table 1 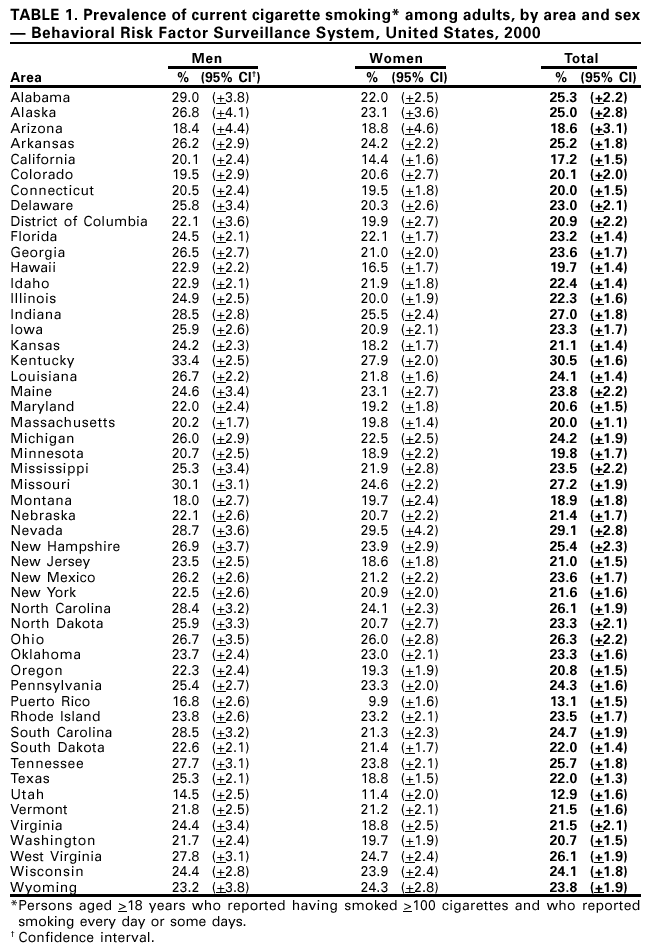 Return to top. Table 2 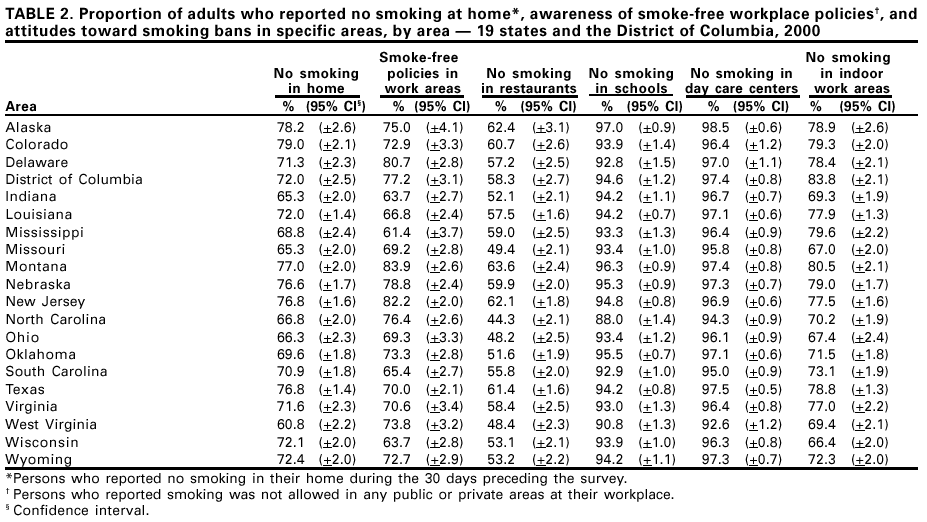 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 12/13/2001 |
|||||||||
This page last reviewed 12/13/2001
|