 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hospital-Based Policies for Prevention of Perinatal Group B Streptococcal Disease --- United States, 1999Please note: An erratum has been published for this article. To view the erratum, please click here. Group B streptococcus (GBS) is the leading cause of sepsis, meningitis, and pneumonia in newborns in the United States (1). Because intrapartum prophylactic antibiotics reduce mother-to-child GBS transmission (2), in 1996, CDC, the American College of Obstetricians and Gynecologists, and the American Academy of Pediatrics recommended that hospitals adopt formal GBS prevention policies (2--4). From 1994 to 1997, the proportion of hospitals with formal intrapartum GBS prevention policies increased from 39% to 59% (5,6); hospitals that implemented policies reported less GBS disease among neonates (7). In 1999, CDC's Active Bacterial Core Surveillance (ABCs) system surveyed hospitals in eight states about their GBS prevention policies. This report summarizes the results of that analysis and indicates that in 1999, the proportion of hospitals with formal policies had not changed since 1997; however, a higher proportion of hospitals have implemented measures to improve policy compliance. From October through December 1999, a structured questionnaire was mailed to hospitals with obstetric services in the metropolitan statistical areas of Atlanta, Georgia (n=30 hospitals; 20 counties); San Francisco, California (n=21; three counties); Albany and Rochester, New York (n=23; 15 counties); Minneapolis/St. Paul, Minnesota (n=19; seven counties); Portland, Oregon (n=13; three counties); Tennessee (n=31; five counties); and Connecticut (n=29) and Maryland (n=35). Nonrespondents were contacted by telephone or fax. Survey responses were analyzed using Epi Info 6.0. Chi-square tests were used to compare 1997 with 1999 survey responses. McNemar's test was used to analyze responses from hospitals that participated in the survey in both years. Some questions were not asked in the 1997 survey; therefore, comparative data were not available. Of the 201 hospitals surveyed in 1999, 187 (93%) responded; 117 (63%) respondents reported having a formal GBS prevention policy, and 97 (86%) of the 117 had written policies. In 1997, 177 (94%) of 189 responded; 103 (58%) of 177 reported having a formal GBS prevention policy, and 82 (80%) of 103 had written policies (Table 1). From 1997 to 1999, 27 (23%) hospitals established new policies and 22 (14%) revised their policies. Of 70 hospitals without policies, 42 (60%) encouraged health-care providers to establish their own policies, and 22 (34%) were developing an institutional policy. Hospitals with policies were larger than hospitals without policies (median births in 1998: 1432 versus 965; p=0.09), and 70 (60%) of 117 had a neonatal intensive care unit (NICU). Twelve (6.4%) of 187 hospitals that had neither a formal policy nor had addressed the issue with providers were less often affiliated with an academic institution than hospitals with poli cies (8% versus 44%; p=0.02) and were less likely to have a NICU (17% versus 60%; p=0.01). Guidelines for GBS prevention recommended one of two strategies to identify pregnant women for intrapartum prophylactic antibiotics: a screening-based approach in which late prenatal cultures are collected and processed, or a risk-based approach in which women are evaluated during labor for obstetric risk factors (e.g., rupture of membranes >18 hours, maternal fever, or prematurity). Of the 117 hospitals with formal policies, 62 (53%) used the screening-based approach, 37 (31%) followed the risk-based strategy, and 16 (14%) reported recommending a combination of risk-based and screening-based strategies (Table 1). Of the hospitals that recommended an agent for intrapartum antibiotics, 87 (80%) of 109 recommended penicillin compared with 56 (60%) of 95 hospitals in 1997 (McNemar's test; p=0.04). In 1999, of the hospitals that recommended an agent for patients allergic to penicillin, 81 (76%) of 106 recommended clindamycin. In 1999, 95 (59%) of 184 hospital laboratories used selective broth media to culture GBS compared with 76 (47%) of 161 laboratories in 1997 (McNemar's test; p=0.11). In 1999, 89 (82%) of 108 hospitals provided information about the GBS policy to physicians and nursing staff; 49 (43%) of 115 provided information to patients. In 1999, 123 (76%) of 162 hospitals that used standardized forms included GBS screening results versus 76 (45%) of 170 hospitals in 1997 (McNemar's test; p=0.016) (Table 2). The use of standing orders for GBS prophylaxis also increased significantly from 65 (37%) of 176 hospitals to 88 (48%) of 182 hospitals in 1999 (McNemar's test; p=0.02). Reported by: P Daily, MPH, L Gelling, MPH, G Rothrock, MPH, A Reingold, MD, Emerging Infections Program, San Francisco; D Vugia, MD, Acting State Epidemiologist, California Dept of Health Svcs. H Linardos, MPH, A Roome, PhD, C Morin, MPH, Q Phan, JL Hadler, MD, State Epidemiologist, Connecticut Dept of Public Health. W Baughman, MSPH, M Farley, MD, D Stephens, MD, Veterans Administration Medical Svcs and Emory Univ School of Medicine, Atlanta; P Blake, MD, State Epidemiologist, Div of Public Health, Georgia Dept of Human Resources. M Pass, MS, L Harrison, MD, Johns Hopkins Univ, Baltimore; JC Roche, MD, Acting State Epidemiologist, Maryland State Dept of Health and Mental Hygiene. J Rainbow, R Lynfield, MD, R Danila, PhD, State Epidemiologist, Minnesota Dept of Health. B Damaske, D Morse, MD, N Bennett, MD, P Smith, MD, State Epidemiologist, New York State Dept of Health. L Duke, K Stefonek, MPH, M Kohn, MD, State Epidemiologist, State Health Div, Oregon Dept of Human Svcs. B Barnes, MS, L Lefkowitz, MD, W Schaffner, MD, Dept of Preventive Medicine, Vanderbilt Medical Center, Nashville; A Craig, Deputy State Epidemiologist, Tennessee Dept of Health. Active Bacterial Core Surveillance, Emerging Infections Program Network, Respiratory Disease Br, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; and an EIS Officer, CDC. Editorial Note:Although the proportion of hospitals with formal GBS prevention policies was unchanged during the study period, neonatal GBS disease declined between 1997 and 1999 (8,9). Increased compliance with hospital policies or increased efforts by health-care providers in hospitals that have no institutional policies may account for this discrepancy (10). Provider surveys in two states indicated that >90% of obstetricians had GBS prevention protocols by 1998 (10). Further decreases in GBS incidence are possible if additional hospitals adopt policies. More hospitals have adopted a systemwide approach to the prevention of GBS; approximately half the hospitals surveyed use standing orders for prophylaxis and one third had forms to simplify recognition of mothers at risk for transmitting GBS to their infants. Documentation of the critical elements of a GBS prevention protocol can facilitate recognition of candidates for intrapartum prophylaxis and improve compliance and policy success. The findings in this report are subject to at least three limitations. First, although the survey achieved a high response rate, hospitals within an active surveillance system were surveyed, and most respondents previously had been surveyed. Second, the policies of these facilities may not be generalizable to hospitals in other locations. Third, the results represent the reported policies of the obstetric programs; the services provided were not measured directly. Antibiotic chemoprophylaxis during the intrapartum period has contributed substantially to the decrease in early-onset GBS disease (8,9). However, with 10%--30% of pregnant women colonized with GBS at any given time (2), continued adherence to prophylaxis recommendations is needed. Improved adherence may be facilitated by educating women about GBS prevention. Educational material and order forms for other information for prenatal-care providers and patients are available on the World-Wide Web, http://www.cdc.gov/ncidod/dbmd/gbs or from CDC's National Center for Infectious Diseases, Division of Bacterial and Mycotic Diseases, Health Communications Activity, A-49, 1600 Clifton Rd, N.E., Atlanta, GA 30333. Orders for multiple copies are available at Public Health Foundation, 1220 L Street, N.W., Suite 350, Washington, DC 20005, telephone (877) 252-1200, or are available on the World-Wide Web, http://www.phf.org. References
Table 1 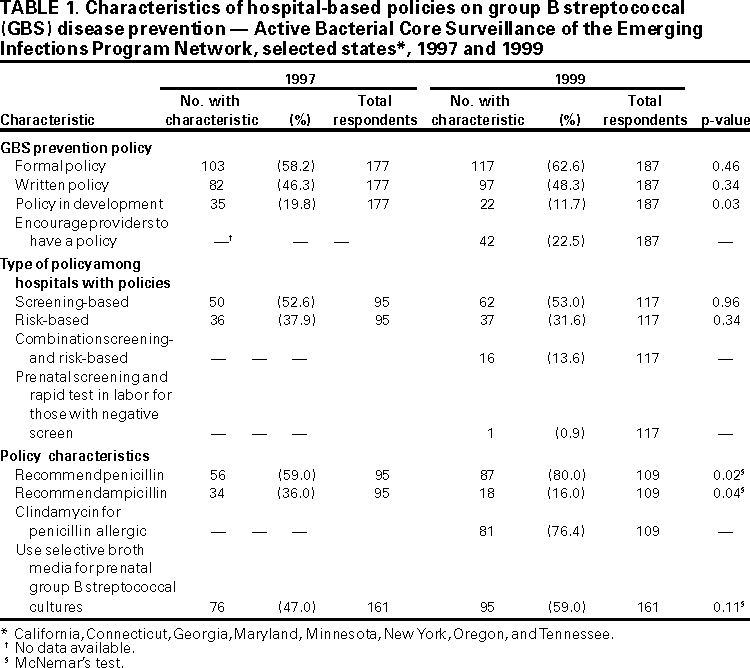 Return to top. Table 2 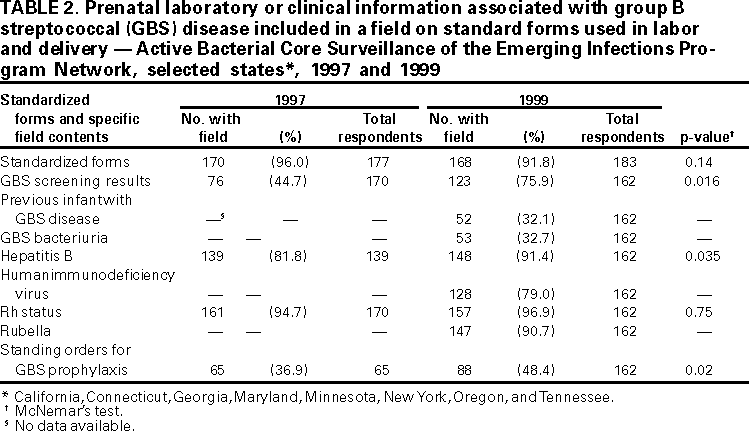 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/19/2000 |
|||||||||
This page last reviewed 5/2/01
|