|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
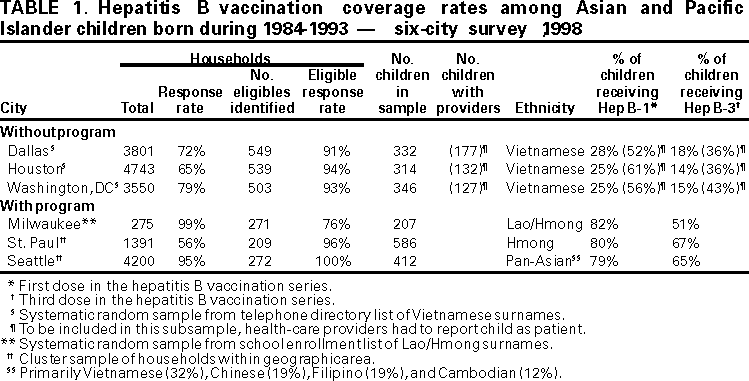
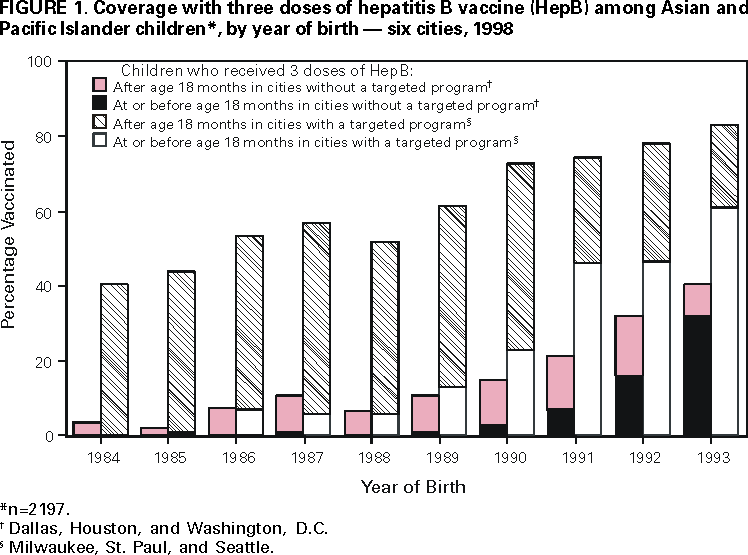
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hepatitis B Vaccination Coverage Among Asian and Pacific Islander Children --- United States, 1998Asian and Pacific Islander (API) children in the United States have high rates of hepatitis B virus (HBV) infection (1--3). To prevent these infections, hepatitis B vaccination has been recommended for these children since the vaccine was first licensed by the Food and Drug Administration in 1981 (4). Recommendations have included universal hepatitis B vaccination of API infants beginning in 1990 and catch-up vaccination for API children aged <7 years (5). These recommendations were reinforced in 1991 when hepatitis B vaccination was recommended for all infants, particularly in populations such as API children with high rates of early childhood HBV infection (6). In 1995, vaccination was recommended for unvaccinated API children aged <11 years and catch-up vaccination for children aged 11--12 years who had not received hepatitis B vaccine (HepB) (7). Series completion among API children aged 19--35 months increased from 39% in 1994 to 88% in 1997 (8). However, among older API children, hepatitis B vaccination coverage was 10% in 1995 (7). In 1998, to examine trends in hepatitis B vaccination catch-up coverage among API children born before 1994, surveys were conducted in six U.S. cities. This report summarizes the results of the surveys, which indicate varying coverage among API children and suggest a need for continued focused vaccination programs for this population. In three cities (Milwaukee, St. Paul, and Seattle), state or county health departments evaluated hepatitis B vaccination programs conducted in the API community. These cities were compared with three other cities (Dallas, Houston, and Washington, D.C.) where no vaccination programs were targeted for API children. Sampling and data collection methods varied between cities. In Milwaukee, students aged 5--14 years with Lao/Hmong surnames were sampled randomly from all public schools. In St. Paul and Seattle, children aged 4--13 and 4--14 years, respectively, were selected using a population-based cluster sample technique. In these three cities, parents or guardians were interviewed in person, and vaccination data were validated with written records from parents, schools, or health-care providers. In Dallas, Houston, and Washington, D.C., a random sample of persons with Vietnamese surnames was selected from area telephone directories, primary caretakers of persons aged 3--18 years were interviewed by telephone, and health-care providers were contacted to verify vaccination histories. For each city, a range of the percentage vaccinated was estimated using the total sample to represent the lower percentage and only those children identified with health-care providers for the higher percentage (Table 1). Children born during 1984--1993 were included for this report. The third HepB dose (HepB-3) was counted if it had been administered at or after age 164 days with an interval of at least 108 days between doses 1 and 3. LOWESS plots (9) were constructed to compare city-specific trends in yearly HepB administration rates among children eligible for vaccination. The percentage of all children in each survey who completed the HepB series by 1998 ranged from 14% (Houston) to 67% (St. Paul) (Table 1). For all children in all surveys combined, the weighted average HepB series completion rate was 42% and did not differ by place of birth (born in the United States versus foreign-born; n=1232 and 708, respectively). Series completion rates at or before age 12, 18, and 60 months were 12%, 16%, and 30%, respectively. Vaccination coverage was examined separately for cities with and without hepatitis B vaccination programs for API children. HepB coverage was 41%--61% and 2%--11% for cities with and without these programs for the 1980s birth cohorts and increased with the 1990s birth cohorts (Figure 1). The increase was greatest in cities with a designated API vaccination program; combined vaccination coverage in the 1993 birth cohort was 83%. The effect of the 1990 and 1991 recommendations for infant vaccination was observed when vaccination coverage was stratified by age at HepB series completion (Figure 1). In each birth cohort, the proportion of children who completed the HepB series by age 18 months (infant vaccination) increased substantially in cities with and without ongoing programs; however, during 1992--1998, annual catch-up vaccination rates as measured by HepB-3 completion remained 7%--11% per year in cities with ongoing API hepatitis B vaccination programs compared with 0.7%--2.6% per year in cities without such programs. Reported by: C Jenkins, Univ of California, San Francisco, California. M Roddy, Minnesota Dept of Health. L Stewart, Seattle-King County Public Health, Seattle, Washington. M Hurie, Wisconsin Div of Health. J Millen, Association of Schools of Public Health, Atlanta, Georgia. Adult Vaccine-Preventable Diseases Br, Epidemiology and Surveillance Div, National Immunization Program, CDC. Editorial Note:The findings in this report document the impact of targeted vaccination programs for populations at high risk for childhood HBV infection. In the three cities with ongoing API hepatitis B vaccination programs, coverage increased with each successive birth cohort over a 10-year period, reaching 83% among children born in 1993; however, in cities without programs, the overall vaccination coverage remained low, although coverage also increased with each successive birth cohort. The three cities with API hepatitis B vaccination programs used three approaches to achieve their higher rates of coverage. In Milwaukee, an active refugee health hepatitis B vaccination program, which began in 1984, provided screening and vaccination services to all new API arrivals. In St. Paul, during the 1989--1991 measles epidemic that resulted in three deaths among Hmong children, a coalition was formed that conducted a multimedia health-promotion campaign and health-care provider education and outreach. In Seattle, state and local health departments and two clinics that served a large proportion of the API population educated providers about the need for catch-up coverage among API children and, during 1996--1997, conducted a 16-month, citywide middle school and high school-based hepatitis B vaccination program for all public school students. The findings in this report are subject to at least three limitations. First, the populations studied may not represent the nationwide API population. Second, the cities with and without programs may not represent all U.S. cities with and without targeted catch-up hepatitis B vaccination programs. Third, biases may have resulted from a loss of randomness in sampling, nonrespondents whose vaccination rates differ from respondents, and missing vaccination records that may have caused inaccurate coverage estimates. Data from the six city surveys and from other cities and state reports (10) indicate that 40% of all API children in the United States aged 7--18 years have completed their HepB series (CDC, unpublished data, 1999). This low rate of coverage in a group at risk for HBV infection underscores the need for increased efforts to continue to provide catch-up vaccination to these children. In addition, catch-up efforts among preschool children are needed in communities where many API infants do not receive HepB. API children born since 1988 who were not vaccinated as infants or caught up as young children should be vaccinated routinely at age 11--12 years. Although eventual high rates of universal adolescent vaccination can be expected for API children living in the 20 states and Washington, D.C., with existing middle school entry laws, special efforts will be needed to ensure vaccination of API children in states without such laws. Because no established vaccination visits exist for older adolescents, hepatitis B vaccination will depend primarily on self-identification, community-based programs, and health-care providers who are aware of the high risk for HBV infection among API children and who can meet specific API cultural and language needs (CDC, unpublished data, 1999). Community-based catch-up hepatitis B vaccination programs have been the mission of the National Task Force on Hepatitis B Immunization, Focus on Asians and Pacific Islanders (on the World-Wide Web at http://aapihp.com*). Successful catch-up initiatives to protect API children should be implemented as quickly as possible. References 1. Franks AL, Berg CJ, Kane MA, et al. Hepatitis B virus infection among children born in the United States to Southeast Asian refugees. N Engl J Med 1989;321:1301--5. 2. Hurie MB, Mast EE, Davis JB. Horizontal transmission of hepatitis B virus infection to United States-born children of Hmong refugees. Pediatrics 1992;89:269--73. 3. Coleman PJ, McQuillan GM, Moyer LA, Lambert SB, Margolis HS. Incidence of hepatitis B virus infection in the United States, 1976--1994: estimates from the National Health and Nutrition Examination surveys. J Infect Dis 1998;178:954--9. 4. CDC. Inactivated hepatitis B virus vaccine. MMWR 1982;31:317--22,327--8. 5. CDC. Protection against viral hepatitis---recommendations of the Immunization Practices Advisory Committee (ACIP). MMWR 1990;39(no. RR-2). 6. CDC. Hepatitis B virus: a comprehensive strategy for eliminating transmission in the United States through universal childhood vaccination. MMWR 1991;40(no. RR-13). 7. CDC. Update: recommendations to prevent hepatitis B virus transmission---United States. MMWR 1995;44:574--5. 8. CDC. Vaccination coverage by race/ethnicity and poverty level among children aged 19--35 months---United States, 1997. MMWR 1998;47:956--9. 9. Cleveland WS. Robust locally weighted regression and smoothing scatterplots. Journal of the American Statistical Society 1979;74:829--36. 10. Euler GL. Changing the legacy for Asian Americans and Pacific Islanders. Asian Am Pacific Isl J Health 1998;6:304--10.
* References to sites of non-CDC organizations on the World-Wide Web are provided as a service to MMWR readers and do not constitute or imply endorsement of these organizations or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of pages found at these sites.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/13/2000 |
|||||||||
This page last reviewed 5/2/01
|