 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Poliomyelitis Eradication -- 1997-1998In 1988, the World Health Assembly resolved to eradicate poliomyelitis globally by 2000 (1). Since then, substantial progress has been reported by all countries where polio is endemic in implementing the recommended polio eradication strategies (i.e., achieving and maintaining high routine coverage with oral poliovirus vaccine [OPV]; conducting National Immunization Days [NIDs]* to rapidly decrease poliovirus circulation; establishing sensitive surveillance systems for polio cases and poliovirus; and carrying out mopping-up vaccination activities to eliminate the remaining reservoirs of poliovirus transmission) (2,3). Although much progress has been made in many countries, substantial obstacles remain, particularly in 14 priority countries (i.e., global reservoir countries** or countries with ongoing armed internal strife or civil war) (Figure 1). This report updates progress during 1998 toward the global eradication target and describes accelerated activities to achieve the 2000 goal. Progress in Implementing Polio Eradication Strategies Routine vaccination. During 1990-1997, reported coverage with three doses of OPV (OPV3) remained at approximately 80% (82% in 1997). Among the World Health Organization (WHO) regions, OPV3 coverage ranged from 82% (Region of the Americas) to 93% (Western Pacific Region) except for the African Region (53%). Supplementary vaccination. During 1998, approximately 470 million children received OPV during NIDs (in 74 countries) and Sub-National Immunization Days (SNIDs)*** (in 16 countries). As of May 1999, only the Democratic Republic of Congo (DR Congo) and Sierra Leone have not conducted full NIDs but did conduct SNIDs in 1998. Liberia, Somalia, and Sudan, areas affected by armed conflict, particularly have been successful in conducting NIDs. In Liberia, approximately 580,000 children were vaccinated twice, in January and March 1999. In Somalia, NIDs covered all areas during August-November 1998, reaching approximately 1.4 million children. In Sudan, NIDs in March and April 1998 and again in March and April 1999 in the conflict zone reached approximately 1 million children who had not been vaccinated during previous NIDs. During intensified NIDs in India in December 1998 and January 1999, 134 million children were vaccinated; door-to-door vaccination was used in high-risk areas (4). Mopping-up. A mopping-up campaign was conducted in adjoining areas of southeastern Turkey, western Iran, northern Iraq, and northeastern Syria during the fall of 1998, reaching approximately 2 million children aged less than 5 years (5). The activity targeted a focus of wild poliovirus transmission in WHO's European and Eastern Mediterranean regions. Turkey is the only country in the European Region to report wild poliovirus in 1998. Acute flaccid paralysis (AFP) surveillance. The objective of AFP surveillance is to detect poliovirus circulation and identify high-risk areas to target for supplementary vaccination; the data also will be used for certification of polio eradication. Two indicators determine the quality of AFP surveillance: 1) the reported rate of AFP not attributable to polio (i.e., nonpolio AFP rate) to assess the sensitivity of case detection and reporting (target: greater than or equal to 1 nonpolio AFP case per 100,000 children aged less than 15 years annually); and 2) the proportion of AFP cases from which two adequate specimens**** have been collected (target: two adequate stool specimens from greater than or equal to 80% of AFP cases). The number of AFP cases reported globally increased substantially from 18,062 cases in 1997 to 24,875 cases in 1998 (Table 1) mainly because of improved AFP surveillance in India. The global nonpolio AFP rate increased from 0.7 per 100,000 population in 1997 to 1.1 in 1998. In the African Region, the nonpolio AFP rate more than doubled from 0.16 in 1997 to 0.42 in 1998. The proportion of AFP cases with two adequate specimens increased globally from 63% in 1997 to 67% in 1998. Only the Western Pacific (86%) and European (78%) regions have reached the levels of stool specimen collection necessary for eradication certification. AFP surveillance has been initiated in all countries where polio is endemic, but is in its early phases in DR Congo, Sudan, and Somalia. AFP reporting is incomplete in many African countries, and stool specimen collection is inadequate, with stool specimens collected for 38% of AFP cases. However, surveillance has improved substantially in many African countries; for example, the number of AFP cases reported in Nigeria increased from five in 1997 to 525 in 1998 (6). The improvement in surveillance indicators in the South-East Asian Region of WHO largely is due to improved reporting from India, where 59 surveillance officers were appointed in late 1997 (4). Global Poliovirus Laboratory Network. By the end of 1998, the Global Poliovirus Laboratory Network expanded to include 117 national and subnational, 15 regional reference, and six global specialized laboratories. Laboratories in the network must be accredited each year by WHO. Overall, 80% of the network laboratories have been reviewed for accreditation, and 80% of these have been fully accredited. Most of the remaining laboratories were accredited provisionally pending subsequent review by the end of 1999. Impact on Polio Incidence As of May 24, 1999, 6227 polio cases with onset during 1998 were reported worldwide (Table 1). This number exceeds the 5185 cases reported in 1997 by 20%. Poliovirus transmission now is confined largely to the remaining major foci of transmission in southern Asia, western Africa, central Africa, and the Horn of Africa. At the end of 1998, poliovirus was suspected or known to circulate in 50 countries, including seven major reservoir countries (Bangladesh, DR Congo, Ethiopia, India, Nepal, Nigeria, and Pakistan), and eight countries in conflict (Afghanistan, Angola, DR Congo, Liberia, Sierra Leone, Somalia, Sudan, and Tajikistan) (Figure 1). The southern Asia reservoir countries reported greater than or equal to 80% of all polio cases globally in 1998. Plans for Acceleration of Polio Eradication To achieve the goal of global polio eradication by 2000, a plan for accelerating polio eradication strategies has been developed by WHO in collaboration with other polio eradication partners. The most important additional activities are 1) in DR Congo and Angola, conducting three rounds of nationwide house-to-house OPV vaccination campaigns in 1999 and 2000 during July-September; 2) in India, carrying out four rounds of intensified NIDs incorporating extensive house-to-house vaccination (called pulse polio immunization) during October 1999-January 2000 and adding two extra rounds of SNIDs each year; and 3) in Pakistan, Bangladesh, Nigeria, and Ethiopia, in addition to NIDs, conducting two extra rounds of house-to-house SNIDs targeting 25%-50% of the target population. Reported by: Vaccines and Other Biologicals Dept, World Health Organization, Geneva, Switzerland. Respiratory and Enterovirus Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Vaccine Preventable Disease Eradication Div, National Immunization Program, CDC. Editorial Note:Three WHO regions have eliminated or are close to eliminating poliovirus--the Region of the Americas has been polio-free since 1991, the Western Pacific Region has not detected poliovirus since March 1997, and poliovirus transmission in the European Region is confined to southeastern Turkey. Reaching the global polio eradication goal will require accelerated activities in the remaining major foci of poliovirus transmission in southern Asia and in Africa. AFP surveillance is not of sufficient quality, particularly in a number of African countries, to assess accurately the effect of supplementary vaccination or target mopping-up vaccination. Additional resources have been made available to African countries, where intense efforts are now under way to enhance surveillance rapidly. The reporting of AFP cases and isolation of wild poliovirus from Afghanistan, Somalia, and Sudan demonstrate the feasibility of AFP surveillance in war-torn countries. Poliovirus transmission is most intense in the major global reservoir countries with large populations--Bangladesh, DR Congo, Ethiopia, India, Nigeria, and Pakistan. With the exception of DR Congo, NIDs have reduced substantially poliovirus circulation in the global reservoir countries. Virologic surveillance in both India and Pakistan demonstrated a large decrease in the biodiversity of circulating polioviruses, indicating a continued reduction in the number of independent chains of transmission. However, poliovirus type 2, usually the first serotype eliminated once effective supplementary vaccination begins, was isolated in 1998 in India, Nigeria, and Pakistan, indicating the continued presence of substantial nonimmune population subgroups in these countries. The observed increase in polio cases from 1997 to 1998 is caused primarily by improvements in AFP surveillance, particularly in India. As reporting becomes more complete, a higher percentage of polio cases is identified and reported, although the actual number of cases probably has decreased substantially. Conflicts in priority countries hinder implementation of polio eradication strategies, particularly vaccination campaigns. Because further delays will endanger reaching the global eradication goal, the polio eradication initiative (PEI) is now focusing much of its resources on key countries in conflict--Afghanistan, Angola, and DR Congo--to assure comprehensive NIDs will be conducted in 1999 and that AFP surveillance systems will be expanded and improved. WHO and the United Nations Children's Fund (UNICEF) have requested that the United Nations assist in negotiating Days of Tranquility for vaccination in DR Congo. Substantial external resources will be required to implement these activities, especially because the PEI focuses on countries that are least able to bear the additional cost. The plan to accelerate polio eradication activities in priority countries calls for increased house-to-house vaccination, which increases the cost per child vaccinated compared with conventional NIDs. Continued support from the polio partnership (Rotary International; CDC; U.S. Agency for International Development; UNICEF; WHO; and the governments of Japan, the United Kingdom, Denmark, and Germany) will be important. New partners, including the United Nations Foundation and the private sector, probably will enhance support in the near future. References
* Nationwide mass campaigns over a short period (days to weeks), in which two doses of OPV are administered to all children in the target age group (usually aged less than 5 years), regardless of vaccination history, with an interval of 4-6 weeks between doses. ** Countries where polio is endemic that have large populations and that may export poliovirus to neighboring countries and elsewhere. *** Focal mass campaigns in high-risk areas over a short period (days to weeks) in which two doses of OPV are administered to all children in the target age group, regardless of vaccination history, with an interval of 4-6 weeks between doses. **** Two stool specimens, collected 24-48 hours apart within 14 days of onset of paralysis, arriving in the laboratory with ice present. Table 1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Acute flaccid paralysis (AFP) and confirmed poliomyelitis,,by World Health Organization region -- 1997-1998*
=======================================================================================================================================
% AFP cases
AFP cases Nonpolio with adequate Confirmed polio cases
reported AFP rate specimens+ (Wild virus confirmed) Wild poliovirus
--------------- ------------ ------------- ------------------------------ strain detected
Region 1997 1998 1997 1998 1997 1998 1997 1998 in 1998
------------------------------------------------------------------------------------------------------------------- in 1998
African 1,203 1,765 0.16 0.42 24% 38% 1,087 ( 31) 992 ( 96) P1/P2/P3
American 1,894 1,608 1.04 0.88 74% 71% 0 ( 0) 0 ( 0) --
Eastern
Mediterranean 2,856 2,213 0.85 0.91 53% 66% 1,255 (264) 536 ( 224) P1/P3
European 1,596 1,534 1.12 1.15 69% 78% 7 ( 6) 26 ( 26) P1/P3
South-East
Asian 4,550 11,358 0.32 1.24 39% 60% 2,827 (531) 4,673 (1,833) P1/P2/P3
Western Pacific 5,963 6,397 1.35 1.43 83% 86% 9 ( 9) 0 ( 0) --
Total 18,062 24,875 0.72 1.10 63% 67% 5,185 (841) 6,227 (2,179)
------------------------------------------------------------------------------------------------------------------- in 1998
* Data reported as of May 24, 1999.
+ Two stool specimens, collected 24-48 hours apart within 14 days of onset of paralysis, arriving in the laboratory with ice present.
=======================================================================================================================================
Return to top. Figure 1 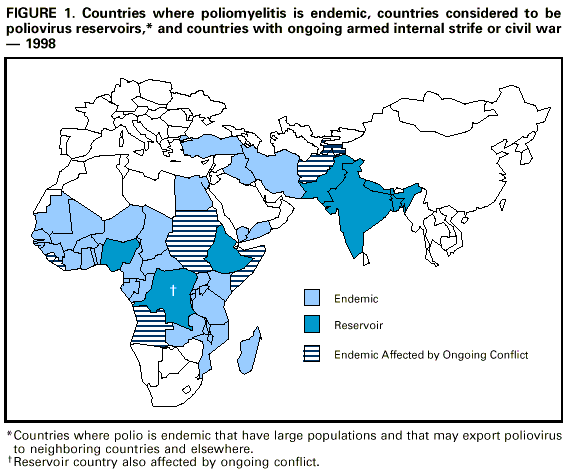 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/27/99 |
|||||||||
This page last reviewed 5/2/01
|