 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
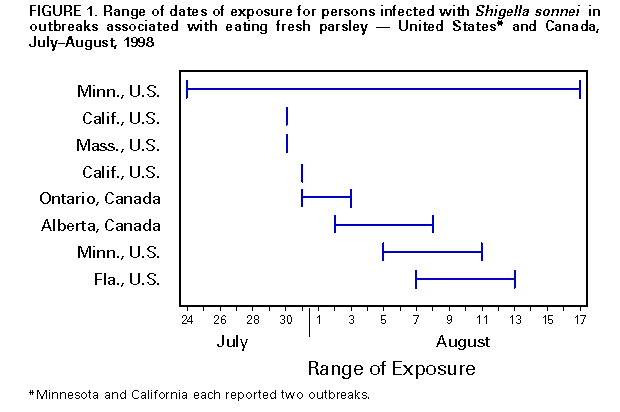
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreaks of Shigella sonnei Infection Associated with Eating Fresh Parsley -- United States and Canada, July-August 1998In August 1998, the Minnesota Department of Health reported to CDC two restaurant-associated outbreaks of Shigella sonnei infections. Isolates from both outbreaks had two closely related pulsed-field gel electrophoresis (PFGE) patterns that differed only by a single band. Epidemiologic investigations implicated chopped, uncooked, curly parsley as the common vehicle for these outbreaks. Through inquiries to health departments and public health laboratories, six similar outbreaks were identified during July-August (in California {two}, Massachusetts, and Florida in the United States and in Ontario and Alberta in Canada). Isolates from five of these outbreaks had the same PFGE pattern identified in the two outbreaks in Minnesota. This report describes the epidemiologic, traceback, environmental, and laboratory investigations, which implicated parsley imported from a farm in Mexico as the source of these outbreaks. United States Minnesota. On August 17, the Minnesota Department of Health received reports of shigellosis in two persons who ate at the same restaurant during July 24-August 17 (Figure_1). S. sonnei subsequently was isolated from stool samples of 43 ill restaurant patrons; an additional 167 persons had probable shigellosis (diarrhea {three or more loose stools during a 24-hour period} lasting greater than or equal to 3 days or accompanied by fever). Eight (18%) of 44 restaurant employees had a similar illness; five had laboratory-confirmed S. sonnei infection. In a case-control study of 172 ill and 95 well restaurant patrons, five items were associated with illness: water (odds ratio {OR}=1.9; 95% confidence interval {CI}=1.0-3.8), ice (OR=3.7; 95% CI=1.6-8.6), potatoes (OR=2.6; 95% CI=1.5-4.6), uncooked parsley (OR=4.3; 95% CI=2.4-8.0), and raw tomato (OR=1.9; 95% CI=1.0-3.9). In a multivariate analysis, only uncooked parsley (OR=4.3; pless than 0.01) and ice (OR=6.9; pless than 0.01) remained significantly associated with illness. California. On August 5, the Los Angeles County Department of Health Services was notified of two persons with shigellosis who ate at the same restaurant on July 31. Stool samples from six ill restaurant patrons yielded S. sonnei; an additional three had probable shigellosis (diarrhea {three or more loose stools during a 24-hour period}, or any loose stools accompanied by fever). All 27 foodhandlers denied illness and had stool samples that were negative for S. sonnei. In an unmatched comparison with 10 well dining companions, ill patrons were significantly more likely to have eaten foods sprinkled with chopped, uncooked parsley (OR=32.0; 95% CI=1.8-1381.4). Massachusetts. On August 11, the Massachusetts Department of Health was notified of six persons who reported illness after eating at a restaurant lunch party on July 30. Stool samples from three persons yielded S. sonnei; an additional three had probable shigellosis (diarrhea within 4 days of the July 30 meal). Chopped, uncooked parsley was served on chicken sandwiches and in cole slaw served at the lunch. In a cohort study of 23 lunch attendees, illness was significantly associated with eating chicken sandwiches (relative risk {RR}=10.0; 95% CI=2.7-37.2) or eating uncooked parsley with any item (RR=10.0; 95% CI=1.4-70.2). All restaurant employees except one submitted a stool sample for culture; all were negative for S. sonnei. Canada On August 10, the Ontario Ministry of Health was notified of a family of three persons with S. sonnei infection who attended a food fair during July 31-August 3. Laboratory-based surveillance identified 32 additional persons with S. sonnei infection who had eaten at a specific kiosk at the fair or at the restaurant that had supplied the kiosk. Of the 35 persons, 20 were questioned about food history; all reported eating a smoked salmon and pasta dish made with fresh chopped parsley. Stool samples from six (38%) of 16 foodhandlers, including the four who handled the parsley, were negative for S. sonnei. One child who had eaten at the kiosk was the index patient at a day care center, from which five secondary cases of shigellosis were reported. Other Investigations In addition to these four outbreaks, four additional restaurant-associated outbreaks of S. sonnei were identified, involving an additional 218 persons with culture-confirmed or probable shigellosis. Of the 111 persons interviewed, 106 (96%) reported eating chopped, uncooked, curly parsley. Isolates from three of these outbreaks (in Minnesota and California in the United States and in Alberta in Canada) matched the outbreak PFGE pattern. In the fourth outbreak (in Florida), one culture-confirmed case was identified; the isolate was not available for PFGE testing. Traceback and Environmental Investigations To determine the source(s) of parsley for the seven outbreaks linked by PFGE, state and provincial health departments, CDC, the Food and Drug Administration (FDA), and the Canadian Food Inspection Agency conducted traceback investigations. Farm A in Baja California, Mexico, was a possible source of parsley served in six of the seven outbreaks; four farms in California were possible sources of parsley in two to four of the seven outbreaks. Field investigations of farm A by FDA and CDC found that the municipal water that supplied the packing shed was unchlorinated and vulnerable to contamination. This water was used for chilling the parsley in a hydrocooler immediately after harvest and for making ice with which the parsley was packaged for transport. Because the water in the hydrocooler was recirculated, bacterial contaminants in the water supply or on the parsley could have survived in the absence of chlorine and contaminated many boxes of parsley. Farm workers and village residents served by this water system reported drinking bottled water or water from other sources. Workers had limited hygiene education and limited sanitary facilities available on the farm at the time of the outbreak. Foodhandlers at six (75%) of the eight implicated restaurants reported washing parsley before chopping it. Usually parsley was chopped in the morning and left at room temperature, sometimes until the end of the day, before it was served to customers. Laboratory Investigations The Minnesota Department of Health laboratory, which has tested isolates of S. sonnei by PFGE routinely since 1995, identified a previously unrecognized PFGE pattern of S. sonnei and a closely related pattern that differed by a single band associated with the two outbreaks in Minnesota. The pattern was distributed to other laboratories through PulseNet, the national molecular subtyping network for foodborne disease. In Minnesota and at CDC, strains from all seven outbreaks for which isolates were available for PFGE testing had the outbreak PFGE pattern. Isolates from the seven outbreaks were resistant to ampicillin, trimethoprim-sulfamethoxazole, tetracycline, sulfisoxazole, and streptomycin. Investigators at the University of Georgia Center for Food Safety and Quality Enhancement conducted studies to determine the effects of temperature and handling on the growth and survival of S. sonnei on parsley. Colony-forming units of S. sonnei per gram (cfu/g) decreased by approximately 1 log per week on parsley, whether chopped or whole, under refrigeration (39 F {4 C}). In contrast, S. sonnei counts increased on parsley kept at room temperature (70 F {21 C}). On whole parsley, the increase was limited to 1 log cfu/g during the first 1-2 days, but on chopped parsley a 3 log cfu/g increase was observed within 24 hours. Reported by: L Crowe, W Lau, L McLeod, Calgary Regional Health Authority; CM Anand, Provincial Laboratory of Southern Alberta; B Ciebin, C LeBer, Ontario Ministry of Health; S McCartney, Ottawa-Carleton Health Unit; R Easy, C Clark, F Rodgers, National Enterics Laboratory, Health Canada; A Ellis, Health Canada; A Thomas, L Shields, B Tate, A Klappholz, I LaBerge, Canadian Food Inspection Agency. R Reporter, H Sato, E Lehnkering, L Mascola, Los Angeles County Dept of Health Svcs, Los Angeles; J Waddell, S Waterman, State Epidemiologist, California Dept of Health Svcs. J Suarez, Miami-Dade County Health Dept, Miami; R Hammond, R Hopkins, State Epidemiologist, Florida Dept of Health. P Neves, Massachusetts Div of Food and Drugs; MS Horine, P Kludt, A DeMaria, Jr, State Epidemiologist, Massachusetts Dept of Public Health. C Hedberg, J Wicklund, J Besser, D Boxrud, B Hubner, M Osterholm, State Epidemiologist, Minnesota Dept of Health. FM Wu, L Beuchat, Center for Food Safety and Quality Enhancement, Univ of Georgia, Athens, Georgia. Food and Drug Administration. Epidemiology Br, Div of Parasitic Diseases; Hospital Environment Laboratory Br, Hospital Infections Program; Foodborne and Diarrheal Diseases Br, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; and EIS officers, CDC. Editorial NoteEditorial Note: S. sonnei is a common cause of gastroenteritis, accounting for 10,262 (73%) of the 14,071 laboratory-confirmed Shigella infections reported to CDC in 1996 (1). Humans and other primates are the only reservoirs for S. sonnei, and transmission occurs through the fecal-oral route. As few as 10-100 organisms can cause infection, enabling person-to-person transmission where hygienic conditions are compromised. In the United States, S. sonnei primarily infects young children and is a common cause of diarrheal outbreaks in child care centers (2). Although reported infrequently, foodborne outbreaks of shigellosis have been associated with raw produce, including green onions (3), iceberg lettuce (4-7), and uncooked baby maize (8). Before the outbreak described in this report, PFGE was not used routinely by most state public health laboratories to subtype isolates of S. sonnei, making it difficult to detect clusters or outbreaks. This investigation demonstrated how the routine use of PFGE and PulseNet can link clusters of S. sonnei infections in widely dispersed geographic areas. This same technology is now used widely for comparing isolates of Escherichia coli O157:H7. CDC, in consultation with the Minnesota Department of Health, is developing a standard protocol for PFGE subtyping of S. sonnei isolates by PulseNet laboratories. In the outbreak described in this report, isolates were resistant to many antimicrobial agents, including ampicillin and trimethoprim-sulfamethoxazole, which are commonly used to treat shigellosis. This highly resistant pattern is seen more frequently in countries other than the United States. During 1985-1995, antimicrobial resistance among Shigella increased substantially in the United States (9): resistance to ampicillin increased from 32% to 67%, resistance to trimethoprim-sulfamethoxazole increased from 7% to 35%, and resistance to both agents increased from 6% to 19%. A history of international travel was the strongest risk factor for Shigella infection resistant to trimethoprim-sulfamethoxazole (9). The findings in this report indicate that several changes in food storage and food preparation procedures are needed. In restaurants, foodhandling practices such as pooling large batches of parsley for chopping and holding chopped parsley at room temperature increase the risk that sporadic low-level bacterial contamination will lead to outbreaks of gastrointestinal illness. When fresh produce is chopped, the release of nutrients may provide a favorable medium for bacterial growth. The risk for outbreaks can be reduced by storing chopped parsley for shorter times, keeping it refrigerated, and chopping smaller batches (10). Changes in parsley production on the farm (e.g., the use of adequately chlorinated water for chilling and icing parsley, education of farm workers on proper hygiene, and possibly the use of post-harvest control measures such as irradiation) may be necessary to ensure that produce is not contaminated with pathogens. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 04/15/99 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}